See 10.5, Isolated Third Cranial Nerve Palsy.
(See Figures 10.6.1 and 10.6.2.)
Figure 10.6.1: Aberrant regeneration of right third cranial nerve showing right-sided ptosis in primary gaze.
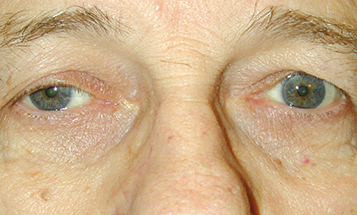
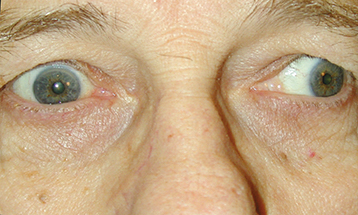
Figure 10.6.2: Aberrant regeneration of right third cranial nerve showing right upper eyelid retraction on attempted left gaze.
The most common signs of aberrant third cranial nerve regeneration include the following:
Eyelid-gaze dyskinesis: Elevation of involved eyelid on downgaze (Pseudo-von Graefe sign) or adduction.
Pupil-gaze dyskinesis: Pupil constricts on downgaze or adduction.
Other signs may include limitation of elevation and depression of eye, adduction of involved eye on attempted elevation or depression, absent optokinetic response, or pupillary light-near dissociation.
Thought to result from misdirection of the third cranial nerve fibers from their original destination to alternate third cranial nerve controlled muscles (e.g., inferior rectus to the pupil).
Aberrancy from congenital third cranial nerve palsies: Can be seen in up to two-thirds of these patients.
Aberrancy from prior acquired third cranial nerve palsies: Seen most often in patients recovering from third cranial nerve damage by trauma or compression by a posterior communicating artery aneurysm.
Primary aberrant regeneration: A term used to describe the presence of aberrant regeneration in a patient who has no history of a third cranial nerve palsy. Usually indicates the presence of a progressively enlarging parasellar lesion such as a carotid aneurysm or meningioma within the cavernous sinus.