Itching, burning, mild pain, foreign body sensation, tearing, erythema of the eyelids, and crusting around the eyes upon awakening. This is in contrast to dry eye syndrome in which symptoms are usually worse later in the day.
Critical
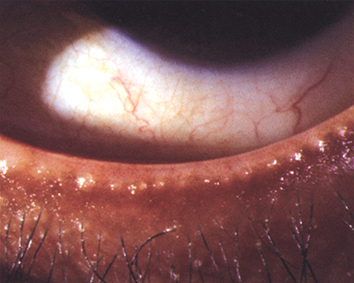
Crusty, red, thickened eyelid margins with prominent blood vessels (see Figure 5.8.1) or inspissated oil glands at the eyelid margins (see Figure 5.8.2). Collarettes, and/or cylindrical sleeves around lashes are indicative of Demodex mites.
Figure 5.8.1: Blepharitis with crusting.
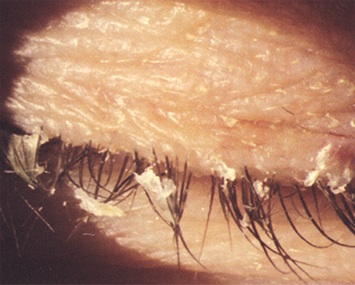
Figure 5.8.2: Meibomitis with inspissated meibomian glands.
Other
Conjunctival injection, swollen eyelids, mild mucous discharge, and SPK. Rosacea may be present. Corneal infiltrates, pannus, and phlyctenules may be present.
See 5.9, Ocular Rosacea, for treatment options in the presence of acne rosacea.
Scrub the eyelid margins twice a day with a commercial eyelid scrub or mild shampoo on a washcloth.
Warm compresses for 5 to 10 minutes b.i.d. to q.i.d.
If associated with dry eyes, use preservative-free artificial tears four to eight times per day.
If moderately severe, add erythromycin ointment or azithromycin gel-drop to the eyelids q.h.s.
Consider omega-3 fatty acid oral supplementation as well as cyclosporine 0.05–0.1%, or lifitegrast 5% drops b.i.d.
Unresponsive meibomitis can be treated with topical ophthalmic antibiotic/steroid ointments (e.g., tobramycin 0.3%/dexamethasone 0.1% or tobramycin 0.3%/dexamethasone 0.05% b.i.d. to t.i.d.). Also consider an oral agent such as doxycycline 100 mg p.o. daily for 1 to 2 weeks; slowly taper to one-fourth full dose and maintain for 3 to 6 months. Oral azithromycin 500 mg/d × 3 days for 3 cycles with 7-day intervals, or 500 mg/d × 1 day followed by 250 mg/d × 4 days, may also be used.
If Demodex mite infestation is suspected, due to the presence of collarettes, and patients have failed the above regimen, consider tea-tree oil eyelid scrubs or an eyelid cleansing agent with hypochlorous acid once or twice daily for a minimum of 6 weeks. Lotilaner 0.25% ophthalmic solution twice daily for 6 weeks is very effective for the treatment of Demodex blepharitis.
If little improvement has been made, consider thermal treatment to the meibomian glands with expression, intense pulsed light therapy, microblepharoexfoliation, and probing of meibomian glands.
|
 NOTE NOTETetracycline derivatives such as doxycycline should not be used in pregnant women, nursing mothers, or children ≤8 years. Azithromycin (see above) or erythromycin 250 mg p.o. b.i.d. are alternatives in these cases. |
|
| NOTE Use azithromycin with caution in patients with cardiovascular disorders (e.g., QT prolongation, proarrhythmic conditions) or with other drugs that prolong the QT interval. |
Two to four weeks depending on the severity of presenting symptoms. Eyelid scrubs and warm compresses may be reduced to once daily as the condition improves but may need to be maintained indefinitely.
|
| NOTE Intractable, unilateral, or asymmetric (not only of eye laterality but also upper versus lower eyelid) blepharitis is rarely a manifestation of sebaceous carcinoma of the eyelid and warrants appropriate clinical workup. See 6.8, Malignant Tumors of the Eyelid. |