Description
- The autonomic nervous system (ANS) regulates individual organ function homeostasis , unlike the somatic nervous system, is not under voluntary control. It comprises the:
- Sympathetic system
- Parasympathetic system
- Enteric nervous system: Not frequently discussed; a meshwork of nerve fibers that innervate the GI tract, pancreas, gallbladder.
- The sympathetic nervous system can be therapeutically blocked via neuraxial techniques (spinal epidural), localized paravertebral ganglia blocks, regional IV sympatholytic injections.
- Sympathetic nervous system (SNS): The SNS is continuously maintaining homeostasis in the body. When stress is encountered there is increased activity resulting in the increased release of catecholamines (“fight or flight”).
- Preganglionic neurons originate in the thoracic lumbar spinal cord. Their axons project to a paravertebral sympathetic trunk (or chain) that extends from C2 to the coccyx. Most preganglionic neurons synapse with postganglionic neurons within the trunk. Some preganglionic neurons travel to other ganglia outside of the sympathetic chain synapse there.
- Postganglionic neurons from the sympathetic trunk (as well as outside ganglia) travel to the target organ.
- Neurotransmitters:
- Effects on organs:
- Eyes: Dilates pupils
- Heart: Tachycardia increased force of contractions (increases systolic blood pressure)
- Vasculature: Increases the tone (vasoconstriction) hence diastolic blood pressure
- Pulmonary: Dilates bronchioles
- Gastrointestinal: Inhibits peristalsis
- Renal: Increases renin secretion which retains sodium water
- Penis: Promotes ejaculation
- Parasympathetic nervous system (PNS): The PNS works complementary to the ANS in maintaining homeostasis in the body. It is generally thought to guide vegetative functions (“rest digest”).
- Preganglion neurons originate in the medulla (cranial nerves III, VII, IX, X) as well as the cervical sacral spinal cord. Their axons project to ganglia close to the target organ where they synapse with postganglionic neurons; they have a longer course compared to preganglionic sympathetic neurons. Of note, 75% of the parasympathetics travel with the vagus nerve.
- Postganglionic neurons have a short distance that they travel to the target organ.
- Neurotransmitters:
- Effects on organs:
- Eyes: Constricts pupils
- Heart: Decreases the heart rate
- Vasculature: Decreases tone (vasodilation)
- Pulmonary: Constricts bronchioles
- Gastrointestinal: Promotes peristalsis
- Penis: Promotes erections
- Adrenal medulla: Develops temly in utero with the SNS acts as a modified sympathetic ganglion. Synapses occur between preganglionic postganglionic neurons within it, but the postganglionic neurons do not leave the medulla; instead they directly release norepinephrine epinephrine into the blood.
Physiology/Pathophysiology
- Complex regional pain syndrome I II is a chronic neuropathic pain disorder. Although the exact pathophysiology remains unknown, manifestations are secondary to ANS dysfunction. CRPS I II are characterized by pain in a nondermatomal pattern. Signs symptoms of neuropathic pain include intense burning pain, hyperalgesia, allodynia, local edema, sweating, skin color changes, temperature disturbances in the affected extremity.
- Peripheral vascular disease refers to arterial obstruction outside the heart. It can cause ischemia is believed to be associated with dysfunction of the ANS.
- Raynaud's disease is an exaggerated reversible vasospasm of digital arteries in response to cold or stress. The etiology is believed to be secondary to ANS dysfunction.
- Propofol, at clinically relevant concentrations for sedation, does not alter central sympathetic outflow at the spinal cord level. However, at deeper levels of sedation induction doses, it can depress central sympathetic activity is likely to lead to hypotension (decreases preload, afterload, contractility).
- Ketamine causes direct, dose-dependent stimulation of the CNS that leads to increased SNS outflow. Consequently, cardiovascular effects resemble SNS stimulation: Increases in systemic pulmonary blood pressures, heart rate, cardiac output, cardiac work, myocardial oxygen requirements. Systemic vascular resistance LV end diastolic pressure are normally unchanged. In the critically ill, it has a negative inotropic effect.
- Etomidate maintains hemodynamic stability through preservation of both sympathetic outflow autonomic reflexes.
- Opioids generally have a dose-dependent sympatholytic effect.
- Benzodiazepines can influence autonomic neurocardiac regulation, probably through their interaction with the gamma-aminobutyric acid A-receptor (GABAA) chloride ion channel complex. They act in a biphasic manner: Initially causing a reduction in central vagal tone followed by decreasing the cardiac pacemaker directly. Induction doses can reduce blood pressure but not to the same degree as propofol.
- Anticholinesterases enhance PNS activity will cause bradycardia, hypotension, hypersecretion, bronchoconstriction, GI tract hypermotility, decrease intraocular pressure.
- Anticholinergics inhibit parasympathetic nerve impulses by selectively blocking acetylcholine receptor binding at nerve junctions.
- Inhaled volatile anesthetics generally suppress the ANS components in a dose-dependent manner.
- Neuraxial blocks: Local anesthetics injected into the epidural or intrathecal space produce a differential blockade. Nerve fibers have different sensitivities due to their location in the spinal cord, diameter, the presence or absence of myelin. Sympathetic nerve fibers are blocked first, are usually followed by pain, sensory, motor nerves.
- Sympathetic blocks: Performed to interrupt nociceptive pathways as well as vasomotor, sudomotor, visceromotor nerves. Low concentrations of local anesthetics block small myelinated A-delta unmyelinated C fibers with a minimal effect on other parts of the peripheral nerves. They may be performed as a diagnostic tool to determine if sympathetic input is a contributor to the pain state. Thus, they help guide decisions on whether a more permanent intervention would be helpful (e.g., neurolysis or surgery).
- Horner syndrome is seen with interscalene brachial plexus blocks, due to the nerve's proximity. Manifests as ptosis, miosis, enophthalmos, conjunctival injection, nasal congestion, facial anhidrosis.
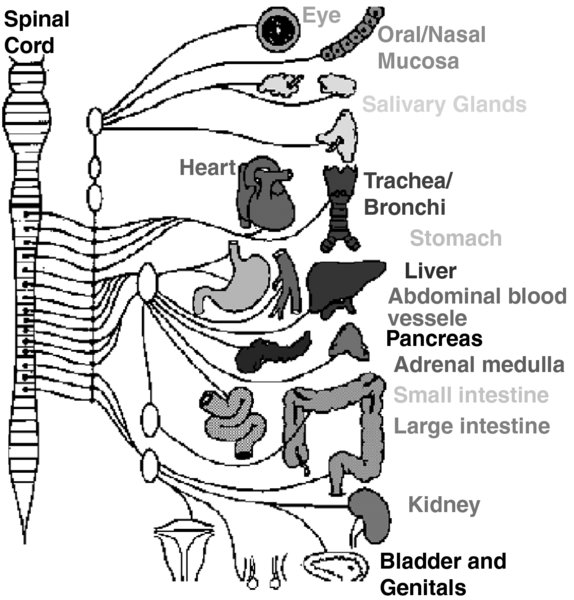
FIGURE 1. Sympathetic nervous system.
Preganglionic neurons originate in the thoracic lumbar spinal cord synpase with postganglionic neurons in the paravertebral sympathetic trunk.

FIGURE 2. Parasympathetic nervous system.
Preganglionic neurons originate in the medulla cervical sacral spinal cord then synapse with postganglionic neurons near the target organ.