▶Neurofibromatosis (NF) is a cluster of syndromes sharing common features.
■NF type 1 (NF1) is transmitted as an autosomal dominant trait (50%) or occurs as a spontaneous pathogenic variant (50%). The gene responsible (NF1 gene) is located on chromosome 17 and encodes the protein neurofibromin.
■Inheritance of NF type 2 (NF2) is autosomal dominant, with 50% spontaneous new pathogenic variants. The gene responsible (NF2 gene) is located on the long arm of chromosome 22 and encodes the protein merlin.
▶NF1
■Two or more of the following clinical features are necessary for the diagnosis of NF1:
– Café au lait macules (Figure 89.1).
Six or more measuring more than 0.5 cm in infants and children or more than 1.5 cm in postpubertal individuals. (The majority of children who have ≥6 café au lait macules ultimately will have NF1 diagnosed.)
Have smooth borders (“coast of California”).
Nearly all patients who have NF1 meet this criterion.
– Two or more neurofibromas of any type (Figure 89.2) or 1 or more plexiform neurofibromas (Figure 89.3).
– Axillary or inguinal freckling (Figure 89.4); occurs in 85% of patients.
– Optic glioma; present in 15% to 20% of pediatric patients with NF1; most commonly detected in those younger than 6 years.
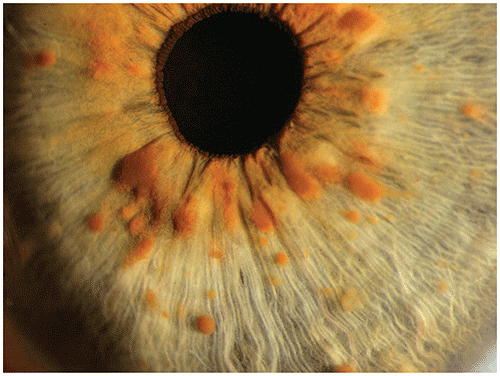
– Two or more Lisch nodules (iris hamartomas); these are rarely seen before 3 years of age (Figure 89.5).
– Characteristic osseous lesion (eg, dysplasia of the sphenoid bone; dysplasia of long bone cortex, which often manifests as anterolateral bowing of long bones [ie, the tibia]; and pseudarthrosis).
– A parent who meets the diagnostic criteria for NF1.
■Other common features observed in patients who have NF1 include the following:
– Macrocephaly (independent of tumors or severity).
– Short stature.
– Precocious puberty.
– Scoliosis.
– Hypertension (may be due to renal artery stenosis or pheochromocytoma).
– Learning disabilities observed in as many as 40% of children; attention-deficit/hyperactivity disorder and autism spectrum disorder also may occur.
– Intellectual disability seen in approximately 5% of patients.
– Epilepsy occurs in as many as 7% of individuals.
▶NF2-related schwannomatosis
■In children, the diagnosis should be suspected when 2 or more of the following are present:
– A schwannoma at any location, including intradermal.
– Skin plaques present at birth or in early childhood (often plexiform schwannomas at histologic examination).
– A meningioma, particularly non-meningothelial (non-arachnoidal) cell in origin.
– A cortical wedge cataract.
– A retinal hamartoma.
– A mononeuropathy, particularly causing a facial nerve palsy, foot or wrist drop, or third nerve palsy.
■Other features include the following:
– Fewer cutaneous neurofibromas than in patients who have NF1.
– Small numbers of large, pale café au lait macules.
Figure 89.1. Multiple Café Au Lait Macules in a Patient Who Has Neurofibromatosis Type 1.
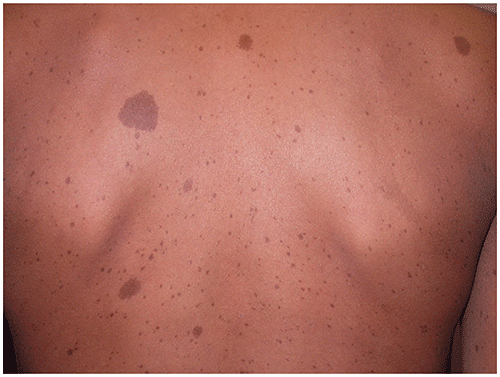
Figure 89.2. Neurofibromas and a Café Au Lait Macule in a Patient Who Has Neurofibromatosis Type 1.

Figure 89.3. Plexiform Neurofibromas (Ie, Large, Subcutaneous Masses [arrows]) in a Patient Who Has Neurofibromatosis Type 1.
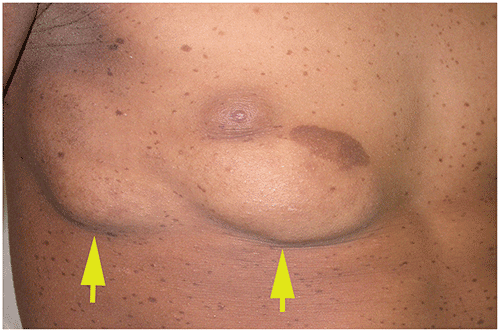
Figure 89.4. Axillary Freckling in a Patient Who Has Neurofibromatosis Type 1.

Figure 89.5. Lisch Nodules (Iris Hamartomas) are Observed in Patients Who Have Neurofibromatosis Type 1.
Look-alikes
The constellation of features observed in patients who have NF1 generally suggests the diagnosis and excludes other disorders. Some other diseases characterized by multiple café au lait macules are presented as follows:
| Disorder | Differentiating Features |
|---|
| McCune-Albright syndrome | Large segmental café au lait macule(s), often with “coast of Maine” (shaggy border) appearance. Bony variations (eg, polyostotic fibrous dysplasia). Endocrine variations.
|
| Silver-Russell syndrome | |
| Bloom syndrome | |
| Multiple café au lait macules without neurofibromatosis | Multiple café au lait macules without other features of neurofibromatosis type 1. Some of these patients may have Legius syndrome (caused by SPRED1 pathogenic variant), characterized by multiple café au lait macules and, in some cases, intertriginous freckling, lipomas, macrocephaly, learning disabilities, attention-deficit/shyperactivity disorder, and developmental delay.
|
▶The diagnosis of NF1 or NF2 is usually made clinically, satisfying the criteria listed previously.
▶Molecular genetic testing is available for NF1 and NF2 and may be used to confirm a clinical diagnosis or evaluate a patient in whom diagnostic uncertainty exists. It may also be used in counseling those affected who are planning a pregnancy or in prenatal diagnosis once pregnant.
▶There is no specific therapy for NF1. Management is directed primarily at identifying and treating complications. Those providing health care for patients who have NF1 should consult the American Academy of Pediatrics clinical report, “Health Supervision for Children With Neurofibromatosis Type 1” (Pediatrics. 2019;143[5]:e20190660). Elements of surveillance include the following:
■Genetic evaluation.
■At all health maintenance visits monitor growth, head circumference, and blood pressure; perform a complete examination concentrating on cardiac, cutaneous, ophthalmologic, neurologic, and skeletal systems; monitor for precocious puberty; and assess development and behavior, vision, and hearing.
■Ophthalmologic examination annually until puberty, then as needed.
■Head magnetic resonance imaging: The role of this procedure (eg, to determine whether an optic glioma is present) in individuals without symptoms is controversial and should be determined on a case-by-case basis in collaboration with an ophthalmologist.
■Selumetinib (an inhibitor of mitogen-activated protein kinase kinase enzyme, or MEK inhibitor) is approved by the US Food and Drug Administration for treatment of children 2 years or older with symptomatic inoperable plexiform neurofibromas).
▶There is no specific therapy for NF2. Management should include the following:
■Genetic evaluation.
■Surveillance for vestibular schwannomas by means of magnetic resonance imaging, audiometry, or brainstem auditory evoked response.
▶NF1: Learning disabilities, optic gliomas, plexiform neurofibromas, and other complications should be addressed if they develop.
▶NF2: Vestibular schwannomas or hearing loss should be addressed if present.
▶The prognosis for NF is variable, depending on the severity of involvement and development of malignancy.
▶The spectrum of severity ranges from individuals with minimal effect on quality of life to those with profound effect or who require multiple procedures and coordinated multispecialty care.
▶NF1: Development of pain in or sudden growth of a plexiform neurofibroma; sudden changes in visual acuity; development of headache, hypertension, scoliosis, or variations of long bones.
▶NF2: Development of hearing loss, tinnitus, difficulties with balance, headache, or other signs of increased intracranial pressure.
▶Subspecialties that may be involved in the care of patients with NF include genetics, neurology, ophthalmology, surgery (ie, orthopedic, general, plastic), dermatology, otolaryngology, and oncology.
▶Children’s Tumor Foundation: Education and links to support and physicians for patients who have NF and their families.
www.ctf.org
▶Neurofibromatosis Consortium: Information about ongoing clinical trials and links to NF clinical centers.
www.uab.edu/nfconsortium
▶Neurofibromatosis Network: Provides support and information for patients and families.
www.nfnetwork.org