Population: Patients with CAD and Type 2 diabetes mellitus.
Organization
 AHA 2020
AHA 2020
Recommendations
–Use an A1c goal of <8.0–8.5.
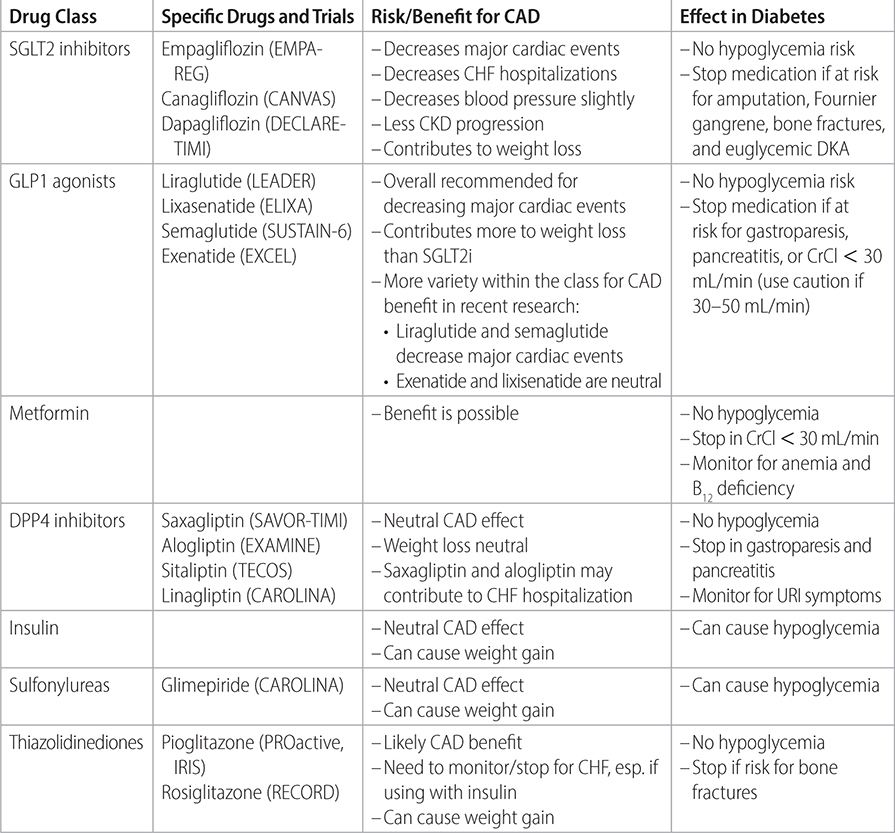
–The use of different medications to attain a glycemic goal can affect CAD-related endpoints. See Table 19–9.
–Antiplatelet therapy: Data is insufficient to give a definitive recommendation.
–Hypertension: BP goals based on combination of comorbidities:
• T2DM + HTN + CAD <140 / <90.
• T2DM + HTN + CAD + stroke risk <130 / <80.
• T2DM + HTN + CAD + CKD/microalbuminuria <130 / <80.
–Benefits/risks of antihypertensive classes in T2DM and CAD:
• ACEi/ARBs: first line. Reduce first and recurrent cardiovascular events; reduce progression of microalbuminuria.
• Long-acting thiazide-like (chlorthalidone/indapamide): second-line option. Increase serum glucose slightly by decreasing insulin sensitivity but unclear if of clinical significance. Has cardiovascular benefit.
• Dihydropyridine CCBs (amlodipine): second-line option. Has cardiovascular benefit and is antianginal.
• Aldosterone antagonists (spironolactone): third-line option. Important in comorbid LV dysfunction or prior MI.
• Beta-blockers: Do not reduce mortality in CAD after 30 days. Can be used in T2DM if there is concurrent chronic angina or if need another agent. Not all beta-blockers have equal benefit. Use carvedilol, labetolol, or nebivolol for vasodilatory effect and neutrality in T2DM. Instead, metoprolol and atenolol will reduce demand but cause peripheral vasoconstriction, which increases insulin resistance and increases LDL.
–Lipids: Use statins for all with CAD and DM.
• If LDL is >70 despite high-intensity statin, consider ezetimibe or PCSK9 inhibitors (evolocumab or alirocumab) for additional risk reduction in death, MI, stroke, or hospitalization.
• If triglycerides are >135 despite statins, consider addition of icosapent ethyl 2g BID which has been shown to decrease cardiovascular death, MI, stroke, CABG, unstable angina.
–Smoking: Stop smoking. The weight gain in T2DM from cessation does not undo the drop in risk of major cardiac event.
–Diet: Recommend a Mediterranean diet with extra virgin olive oil or mixed nuts saw benefit for reduction in major cardiac events or stroke.
–Activity: Recommend 150 min/wk of moderate to vigorous physical activity. Refer to cardiac rehabilitation after the first major cardiac event, as the intervention has been shown to be preventative of future cardiac events if tailored to T2DM.
–Weight loss: Diet and exercise have modest benefit in CAD and T2DM. Liraglutide has been shown to decrease weight (see Table 19–9) and improve CAD outcomes. Bariatric surgery has been shown to better control CAD risk factors (glycemic control, LDL, triglycerides, HTN) but not necessarily to improve CAD endpoints.
TABLE 19–9 DIABETES MEDICATIONS WITH CARDIOVASCULAR BENEFITS
Practice Pearls
• Intensive glycemic control A1c < 6.0%–7.0% has not been shown to decrease major cardiac events, though glycemic control <7.0% does show some benefit for microvascular consequences of diabetes such as blindness, microalbuminuria, ESRD, and distal neuropathies.
• T2DM is a generalized prothrombotic state, especially when exacerbated by CKD. Responsiveness to DAPT may be impaired. Clopidogrel alone may be reasonable compared to aspirin alone in T2DM w/ prior MI, ischemic stroke, or PAD. At this time, large trials have not shown benefit when antithrombotic regimens are adjusted based on platelet function testing.
• 70%–80% of patients with T2DM also have HTN. This increases the risk of MI, stroke, and all-cause mortality. Intensive control of systolic blood pressure in this group <130 decreases risk of stroke, but has no benefit in decreasing coronary events. There are increased risks of adverse events in too much control of HTN in CAD.
• The ACCORD trial demonstrated that 30% of T2DM need 2 antihypertensives, 39% of T2DM need 3 antihypertensives.
• Statins have significant benefit in primary and secondary CAD prevention and patients with T2DM. Studies have shown that statins can cause small increase in incident T2DM, but the risk is lower than with thiazides or non-vasodilating BB; the protective benefit of statins in T2DM is more substantive and favors administration.
• Stress: Patients with T2DM have increased risk for stress and depression. This has been shown to increase risk of stroke. Stress in T2DM has been shown to increase risk of major cardiac event. The mechanisms are unknown. It is unknown if decreasing stress/depression then resolves the increased risk.
Source
–Circulation. 2020;141:e779-e806.