Population: Children age 3 mo to 18 y with acute otitis media.
Organization
 AAP 2013
AAP 2013
Recommendations
Evaluation
–Make diagnosis in children with an effusion and on one of the following findings:
• Moderate or severe TM bulging.
• Mild bulging and onset of ear pain in the past 24 h.
• Erythema of the TM.
• New onset of otorrhea not caused by otitis externa.
Management
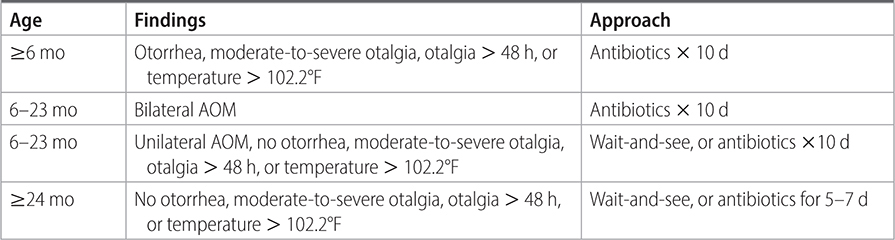
–See Table 22–1 for treatment approaches based on age and findings.
TABLE 22–1 ACUTE OTITIS MEDIA—APPROACHES TO TREATMENT
–Educate caregivers about prevention of otitis media: encourage breast-feeding, feed child upright if bottle fed, avoid passive smoke exposure, limit exposure to groups of children, careful handwashing prior to handling child, avoid pacifier use >10 mo, ensure immunizations are up to date.
–Provide symptomatic relief with acetaminophen, ibuprofen, and warm compresses to the ear.
–Use amoxicillin as the first-line antibiotic for low-risk children.
–Use alternative medication if failure to respond to initial treatment within 72 h; penicillin allergy; presence of a resistant organism found on culture.
–Refer to an ear, nose, and throat (ENT) specialist for any complications of otitis media including mastoiditis, facial nerve palsy, lateral sinus thrombosis, meningitis, brain abscess, or labyrinthitis.
–Do not require routine rechecks at 10–14 d for children feeling well.
–Do not routinely prescribe antibiotics in children age 2–12 y with nonsevere AOM when observation is an option.
Practice Pearls
• Amoxicillin is first-line therapy for most children.
- 80–90 mg/kg/d in 2 divided doses.
• Use amoxicillin-clavulanate if child has received antibiotics in prior 30 d.
• Alternative antibiotics:
- Amoxicillin-clavulanate.
- Ceftriaxone.
- Cefprozil.
- Loracarbef.
- Cefdinir.
- Cefixime.
- Cefpodoxime.
- Azithromycin.
- Erythromycin.
Sources
–Pediatrics. 2013;131:e964-e999.
–http://www.choosingwisely.org/societies/american-academy-of-family-physicians/
–Am Fam Physician. 2013;88(7):435-440.