AUTHORS: Betelhem Kifle, MD and Lekshmi Santhosh, MD, MAEd




Definition
Viral pneumonia is a lung infection caused by any of a large number of viral pathogens. Some of the most important viruses are discussed in this chapter.
Epidemiology & Demographics
Incidence (in U.S.)
- COVID-19 (SARS-CoV-2 virus):
- Influenza virus:
- The CDC estimated ∼13 million illnesses, ∼6.1 million medical visits, 170,000 hospitalizations, and ∼14,000 deaths caused by influenza in the 2021 to 2022 influenza season.1
- Secondary bacterial pneumonia develops in a small percentage of infected persons.
- Incidence of other important viral pathogens can vary widely depending on setting, geography, and testing modalities. With the more widespread use of rapid molecular testing of respiratory secretions, an increase in the detection of viral pathogens has been observed. However, determining causality of the identified virus to the suspected pneumonia remains challenging because respiratory viruses remain detectable for several weeks after initial infection, and the pneumonia may be due to secondary bacterial infection.
Predominant Age
- COVID-19:
- Influenza:
- RSV and parainfluenza virus:
- Human metapneumovirus:
- Adenoviruses:
- Varicella:
- Measles:
- Young adults and older children who only received a single vaccination (5% failure rate)
- Currently most cases are seen in unvaccinated individuals
- Measles during pregnancy more likely to be complicated by pneumonia
- Underlying cardiopulmonary diseases and immunosuppression predispose to serious pneumonia
- Before availability of measles vaccine, 90% of pneumonias in those <10 yr
- ∼6% of measles cases are complicated by pneumonia
- Cytomegalovirus (CMV):
Peak Incidence
Genetics
- Close contact, not genetics, is important in acquisition
- Congenital anomalies and immunosuppression worsen course of RSV pneumonia
- CMV is the most common intrauterine infection in the U.S.
- Pneumonia occurs occasionally in infants with symptomatic congenital infection
Physical Findings & Clinical Presentation
- COVID-19: Wide range, from mild symptoms to severe illness
- Influenza:
- RSV, parainfluenza, and human metapneumovirus:
- Fever
- Tachypnea
- Prolonged expiration
- Wheezes and rales
- Diarrhea2
- Adenoviruses:
- Measles:
- Varicella:
- Fever
- Maculopapular or vesicular rash (all lesions at the same stage) becomes encrusted
- Pneumonia typically 1 to 6 days after rash appears. Pneumonia (Fig. E1) may be accompanied by cough and occasionally hemoptysis
- Few auscultatory abnormalities noted on examination of the lungs
- CMV:
Figure E1 This Chest Radiograph Demonstrates Bilateral Nodular and Interstitial Pneumonia Characteristic of Varicella Pneumonia
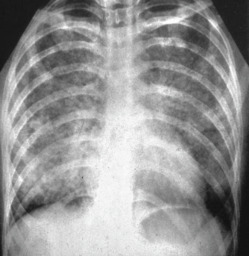
The patient, a 27-yr-old gravida 6, para 2, abortus 3, was exposed to varicella infection in her two children. Characteristic skin vesicles of varicella occurred several days before the development of pulmonary symptoms. She required endotracheal intubation and mechanical ventilation for 6 days. She was treated with intravenous acyclovir and ceftazidime for possible superimposed infection. The patient recovered fully and delivered a healthy infant at term.
From Gabbe SG: Obstetrics, ed 6, Philadelphia, 2012, Saunders.