Definitions
Iridodialysis: Disinsertion of the iris from the scleral spur. Elevated IOP can result from trabecular meshwork damage and/or formation of peripheral anterior synechiae.
Cyclodialysis: Disinsertion of the ciliary body from the scleral spur. Increased uveoscleral outflow occurs initially resulting in hypotony. IOP elevation can later result from closure of a cyclodialysis cleft, leading to glaucoma.
Symptoms
Usually asymptomatic unless glaucoma or hypotony/hypotony maculopathy develop. Large iridodialyses may be associated with monocular diplopia, glare, and photophobia. Both are associated with blunt trauma or penetrating globe injuries. Typically, unilateral.
Signs
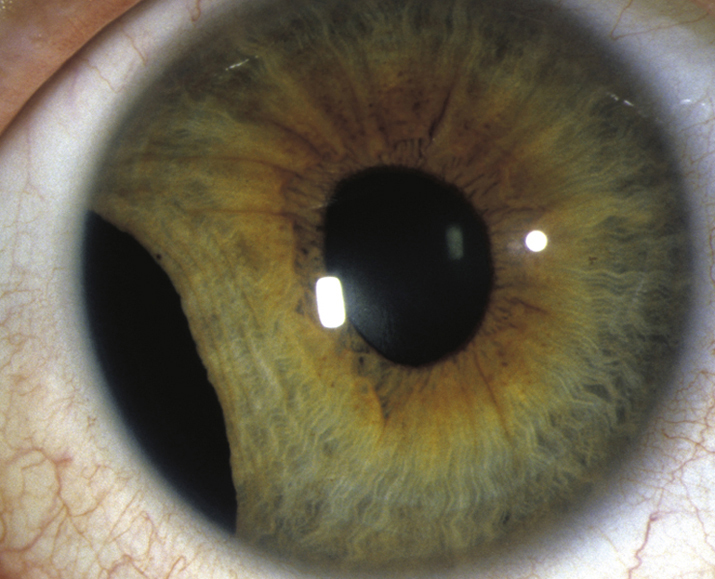
(See Figure 3.7.1.)
Critical
Characteristic gonioscopic findings as described above.
Other
Decreased or elevated IOP, glaucomatous optic nerve changes (see 9.1, PRIMARY OPEN ANGLE GLAUCOMA), angle recession, and hypotony syndrome (see 13.11, HYPOTONY SYNDROME). Other signs of trauma include hyphema, cataract, and pupillary irregularities.
Differential Diagnosis
In setting of glaucoma, see 9.1, PRIMARY OPEN ANGLE GLAUCOMA.
Workup
Treatment
- Sunglasses, contact lenses with an artificial pupil, or surgical correction if large iridodialysis and patient symptomatic.
- If glaucoma develops, treatment is similar to that for primary open angle glaucoma (see 9.1, PRIMARY OPEN ANGLE GLAUCOMA). Aqueous suppressants are usually first-line therapy. Miotics are generally avoided because they may reopen cyclodialysis clefts, causing hypotony. Strong mydriatics may close clefts, resulting in pressure spikes. Often these spikes are transient and easily controlled with topical therapy, as the meshwork resumes aqueous filtration after several hours.
- If hypotony syndrome develops due to cyclodialysis clefts, first-line treatment is usually atropine b.i.d. to reapproximate the ciliary body to the sclera and steroids to decrease inflammation. Further surgical treatment is described in Section 13.11, HYPOTONY SYNDROME.
Follow Up
- See 9.1, PRIMARY OPEN ANGLE GLAUCOMA.
- Carefully monitor both eyes due to the high incidence of delayed open-angle and steroid-response glaucoma in the traumatized eye and an approximately 50% risk of open-angle glaucoma in the uninvolved eye.