Binocular diplopia and ptosis; with or without pain.
 NOTE: NOTE: |
Pain does not distinguish between microvascular infarction and compression. |
Binocular diplopia and ptosis; with or without pain.
| NOTE: |
Pain does not distinguish between microvascular infarction and compression. |
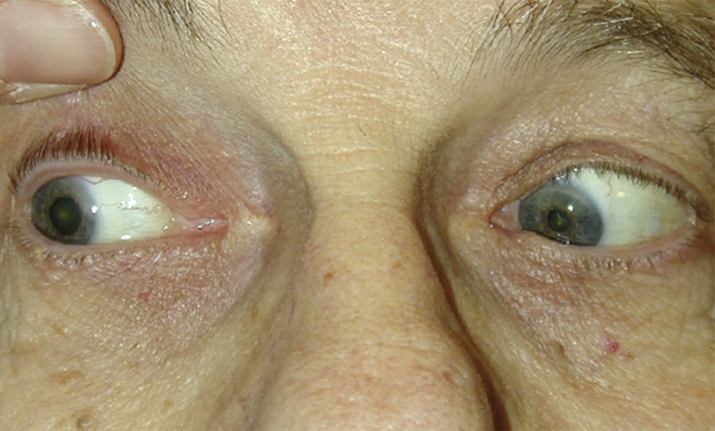
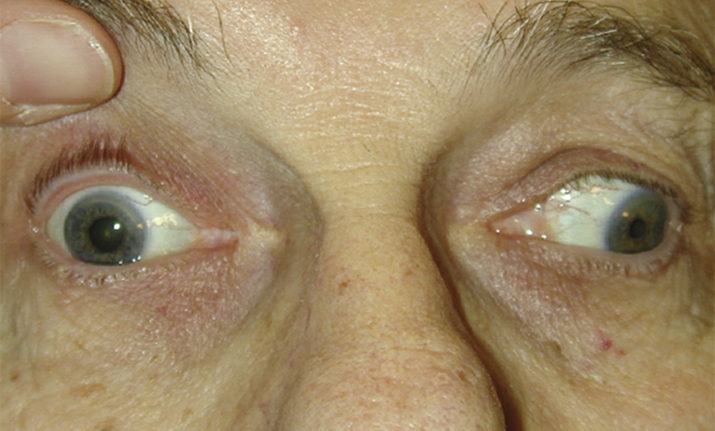
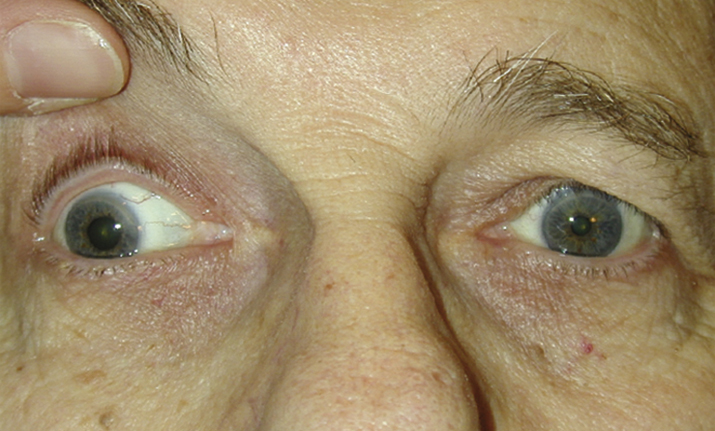
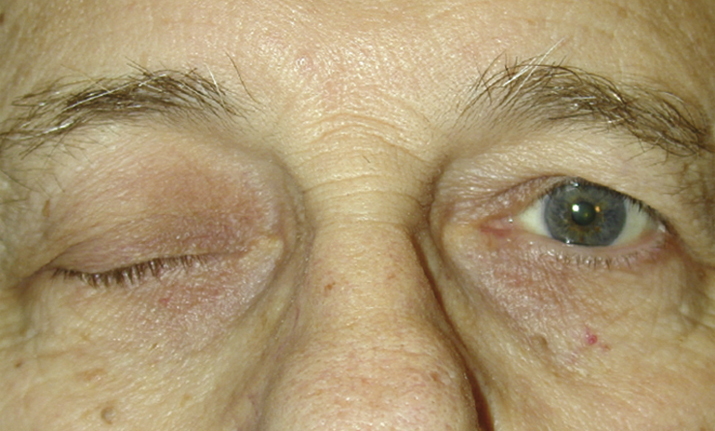
(See Figures 10.5.1 to 10.5.4.)
Critical
Other
An exotropia or hypotropia. Aberrant regeneration. See 10.6, ABERRANT REGENERATION OF THE THIRD CRANIAL NERVE.
| NOTE: |
The ipsilateral fourth cranial nerve can be assessed by focusing on a superior conjunctival blood vessel and asking the patient to look down. The eye should intort, and the blood vessel should turn down and toward the nose even if the eye cannot be adducted. |
| NOTE: |
Most sensitive modality to identify aneurysm is contrast-enhanced CTA, though MRA is also very sensitive and can be done if CTA is contraindicated or unavailable. Gadolinium-enhanced MRI is most sensitive for identifying mass lesions and inflammatory etiologies. Choice of imaging should be made in conjunction with neuroradiology. If initial imaging studies are negative but clinical suspicion remains high, catheter angiography may be indicated. |