(See Figure 6.9.1.)
Critical
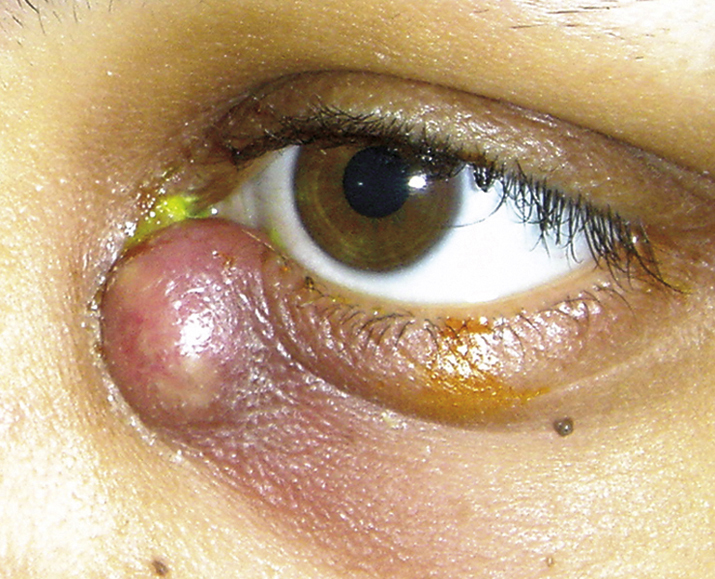
Erythematous, tender, tense swelling over the nasal aspect of the lower eyelid and extending around the periorbital area. Mucoid or purulent discharge can be expressed from the punctum when pressure is applied over the lacrimal sac.
 NOTE: NOTE: |
Swelling in dacryocystitis is below the medial canthal tendon. Suspect lacrimal sac tumor (rare) if the mass is above the medial canthal tendon. |
Other
Fistula formation from the skin below the medial canthal tendon. A lacrimal sac cyst or mucocele can occur in chronic cases. Progression to a lacrimal sac abscess, and rarely, orbital or facial cellulitis may occur.