(see Figure 6.10.1.)
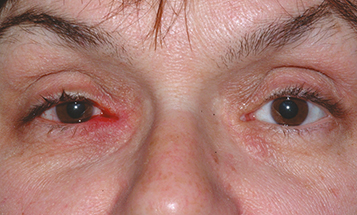
Erythematous “pouting” of the punctum (turned outward) and erythema of the surrounding skin. Expression of mucopurulent discharge or concretions from the punctum is diagnostic.
Recurrent conjunctivitis confined to the nasal aspect of the eye, gritty sensation on probing of the canaliculus, and focal injection of the nasal conjunctiva.