(See Figure 12.14.1.)
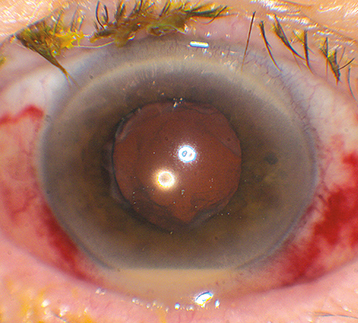
Hypopyon, fibrin, severe AC reaction, vitreous cells and haze, and decreased red reflex.
Eyelid edema, corneal edema, intense conjunctival injection, chemosis (all are highly variable).
Organisms
Sudden onset of decreased vision and increasing eye pain after surgical procedure. Usually within 1 to 2 weeks of ocular surgery.
(See Figure 12.14.1.)
Hypopyon, fibrin, severe AC reaction, vitreous cells and haze, and decreased red reflex.
Eyelid edema, corneal edema, intense conjunctival injection, chemosis (all are highly variable).
Organisms
Toxic anterior segment syndrome (TASS): Occurs 6 to 24 hours after cataract surgery. Diffuse corneal edema with KP. Due to endotoxin from surgical instruments or fluids. Usually responds to intensive topical steroid and cycloplegic therapy but may require endothelial keratoplasty or penetrating keratoplasty for persistent corneal edema.
Acute noninfectious uveitis flare: Ask about history of previous uveitis; HLA-B27–associated anterior uveitis may be precipitated by trauma, including surgery.
Sterile (noninfectious) endophthalmitis (e.g., following intravitreal triamcinolone acetonide or anti-vascular endothelial growth factor [VEGF] injection).
Lens-particle uveitis (retained lens fragment in the angle or vitreous or retained lens cortex in the capsular bag).
See also 12.15, Subacute and Chronic Postoperative Uveitis.
Complete ocular history and examination. Look for wound/bleb leak, exposed suture, vitreous to wound, blepharitis, or other predisposing factors for endophthalmitis.
Consider B-scan US if there is limited view of the posterior segment, which may confirm marked vitritis and/or membrane formation and establishes a baseline against which the success of therapy can be measured.
If vision is light perception postcataract extraction, a diagnostic and therapeutic vitrectomy is often indicated. Cultures (blood, chocolate, Sabouraud, and thioglycolate) and smears (Gram and Giemsa stains) should be obtained and intravitreal antibiotics are given. If vision is hand motion or better, vitreous aspiration, or an AC paracentesis if the vitreous specimen cannot be obtained, of 0.2 mL is performed and variably sent for culture. See Appendix 13, Anterior Chamber Paracentesis.
Prevention: Preparation of the conjunctiva with 5% povidone-iodine in all cases and the eyelids for incisional eye surgery prior to surgery has been proven to reduce the risk of endophthalmitis. Intraoperative (e.g., intracameral) antibiotics have also been shown to reduce endophthalmitis risk. While perioperative use of topical broad-spectrum antibiotics may decrease bacterial load, it has not been proven to lower the rates of endophthalmitis and may promote antibiotic resistance.
AC or vitreous tap for Gram stain, culture, and sensitivities along with timely intravitreal injections using broad-spectrum antibiotics (often vancomycin and ceftazidime, or amikacin if penicillin allergic). See Appendix 11, Intravitreal Tap and Inject and Appendix 12, Intravitreal Antibiotics. Consider intravitreal steroids (e.g., dexamethasone 0.4 mg/0.1 mL) in select cases with severe vitreous inflammation.
Consider intensive topical steroids (e.g., prednisolone acetate 1% q1h around the clock) for control of anterior segment inflammation.
Consider intensive topical fortified antibiotics (e.g., vancomycin and tobramycin, q1h around the clock for 24 to 48 hours) in the setting of filtering blebs, wound leaks, or exposed sutures. See Appendix 9, Fortified Topical Antibiotics/Antifungals.
For postcataract extraction endophthalmitis, immediate pars plana vitrectomy is beneficial if visual acuity on presentation is light perception or worse. Vitrectomy for other causes of endophthalmitis (bleb-related, post-traumatic, or endogenous) may be beneficial in select cases.
Systemic antibiotics may be considered. Intravenous antibiotics are not routinely used. Consider i.v. fluoroquinolones (e.g., moxifloxacin) in special circumstances (e.g., bleb-related endophthalmitis or traumatic endophthalmitis). Some oral antibiotics (e.g., moxifloxacin 400 mg p.o. daily) may reach therapeutic vitreous levels and could be considered as alternatives to intravenous antibiotics.
Subconjunctival antibiotics (vancomycin and ceftazidime) were used in the Endophthalmitis Vitrectomy Study; however, their use has become less common.
Relief of pain is a useful early sign of response to therapy.
Early prednisone 60 mg p.o. daily for 5 days was part of the Endophthalmitis Vitrectomy Study protocol. However, its use depends on the causative organism, the patient’s comorbidities (e.g., diabetes, hypertension), as well as the severity and duration of the disease. Once the infection is sterilized, postendophthalmitis inflammation may be significant and should be treated with aggressive topical and occasionally oral steroids.
After 48 hours, patients should show clinical improvement (e.g., relief of pain, decreased inflammation, and decreased hypopyon). Consider reinjecting antibiotics if there is no improvement or if Gram stain shows an unusual organism (targeted at that organism). Consider vitrectomy if the patient is deteriorating.
The antibiotic regimen is refined according to the treatment response, culture results, and culture sensitivity.
If the patient is responding well, topical antibiotics and steroids may be slowly tapered. Close outpatient follow-up is warranted.