(See Figures 11.16.1 and 11.16.2.)

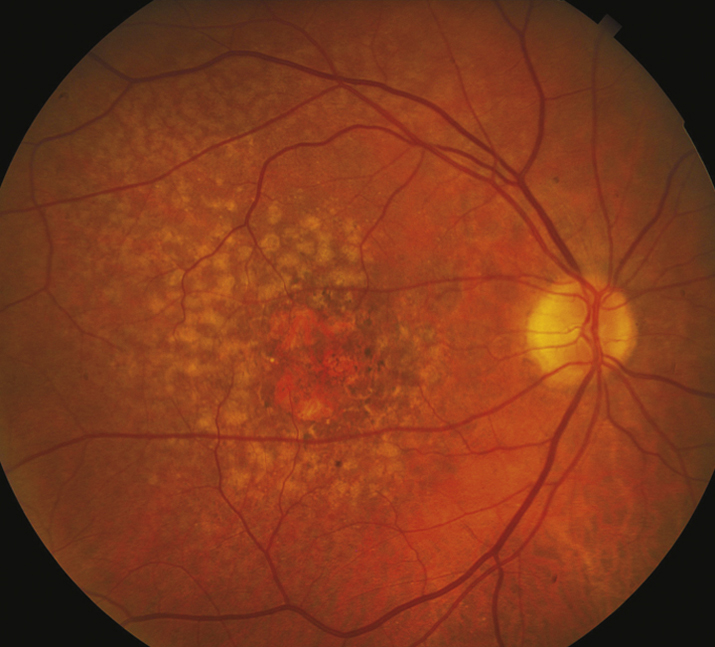
Macular drusen, clumps of pigment in the outer retina, and RPE atrophy, almost always in both eyes.
Confluent retinal and choriocapillaris atrophy (e.g., geographic atrophy [GA]), dystrophic calcification.
(See Figures 11.16.1 and 11.16.2.)
Macular drusen, clumps of pigment in the outer retina, and RPE atrophy, almost always in both eyes.
Confluent retinal and choriocapillaris atrophy (e.g., geographic atrophy [GA]), dystrophic calcification.
Peripheral/extramacular drusen: Drusen only located outside of the macular area. Benign, of no visual significance.
Myopic degeneration: Characteristic peripapillary changes and macular changes without drusen. See 11.22, Pathologic/Degenerative Myopia.
CSCR: Serous retinal elevation, RPE detachments, and mottled RPE, without drusen, hemorrhage, or exudate, usually in patients <50 years of age. See 11.15, Central Serous Chorioretinopathy.
Inherited central retinal dystrophies: Stargardt disease, pattern dystrophy, Best disease, others. Variable macular pigmentary changes, atrophy, or accumulation of lipofuscin or a combination of these. Usually <50 years of age, without drusen, familial occurrence. See specific entities.
Toxic retinopathies (e.g., chloroquine toxicity): Mottled hypopigmentation with ring of hyperpigmentation (bull’s eye maculopathy) without drusen. Possible history of drug ingestion or exposure.
Crystalline retinopathies: A group of heterogenous disorders (e.g. iatrogenic, inflammatory, genetic, toxic, degenerative) associated with crystalline deposits in any layer of the retina. See 11.33, Crystalline Retinopathy.
Inflammatory maculopathies: Multifocal choroiditis, rubella, serpiginous choroidopathy, and others. Variable chorioretinal atrophy, often with vitreous cells and without drusen. See specific entities.
History: Presence of risk factors (e.g., family history, smoking)? See risk factors for loss of vision, 11.17, Neovascular or Exudative (Wet) Age-Related Macular Degeneration.
Amsler grid or preferential hyperacuity perimetry (PHP) testing at home to detect central or paracentral scotoma potentially indicative of neovascular transformation. See Appendix 4, Amsler Grid.
Macular examination with a handheld lens: Look for risk factors for conversion to the exudative form, such as soft drusen or pigment clumping. On OCT, look for reticular pseudodrusen (subretinal drusenoid deposits) as this has been shown to increase risk of conversion to advanced AMD, both neovascular and GA. Look for GA. Look for signs of exudation including edema, SRF, lipid exudation, or hemorrhage (disappearance of drusen may herald the development of CNV).
Baseline and periodic FAF may be useful to monitor for progression of GA.
IVFA or OCT can be useful adjuncts to determine stage of dry AMD and when exudative AMD is suspected based on subjective or objective change in vision or examination findings. Drusen and RPE atrophy are often more visible on IVFA and FAF. OCTA is also a potentially useful diagnostic test as a noninvasive substitute for IVFA or if IVFA is inconclusive, especially with masquerade conditions such as pattern dystrophy or CSCR.
Patients with intermediate dry AMD (one large druse [125 microns] and/or ≥20 medium drusen [63 to 125 microns]), or GA or exudative AMD in one eye but not the other eye, are at high risk for development of advanced stages of AMD. The original Age-Related Eye Disease Study (AREDS) report demonstrated that treatment with a vitamin/mineral formula consisting of vitamin C (500 mg), vitamin E (400 IU), beta-carotene (15 mg), zinc (80 mg), and cupric oxide (2 mg) reduces the risk of progression to advanced AMD by approximately 25% over 5 years and reduces the risk of vision loss caused by advanced AMD by approximately 19% by 5 years. A second study (AREDS2) evaluated the role of increased intake of different carotenoids (lutein and zeaxanthin) as well as two specific omega-3 long-chain polyunsaturated fatty acids (docosahexaenoic acid [DHA] + eicosapentaenoic acid [EPA]). The addition of lutein + zeaxanthin, DHA + EPA, or both to the original AREDS formulation did not further reduce risk of progression to advanced AMD but was found to be equally effective.
Complement inhibitors: intravitreal pegcetacoplan 15 mg and avacincaptad pegol 2 mg (both FDA approved). Consider for patients with GA threatening central vision.
In addition, recommend consumption of dark green leafy vegetables if approved by a primary care physician (intake of vitamin K decreases effectiveness of warfarin) and foods containing high levels of omega-3 fatty acids such as cold-water fatty fish and nuts.
Low-vision aids may benefit patients with bilateral vision loss.
Refer to an internist for management of presumed risk factors: HTN, hypercholesterolemia, smoking cessation, etc.
Those at high risk for progressing to exudative AMD may benefit from home monitoring technology for earlier detection such as the PHP device as well as home OCT. Early detection of CNV increases the likelihood of better visual acuity results after intravitreal anti-VEGF therapy is initiated.
Certain genetic mutations confer an increased risk for AMD (e.g., polymorphisms of complement factor H and ARMS2 genes). This may or may not influence response to treatment and so, at this time, genetic screening in AMD patients is not routinely performed.