Unilateral, painless, acute vision loss (counting fingers to light perception in 94% of eyes) occurring over seconds; may have a history of transient visual loss (amaurosis fugax).
(See Figure 11.6.1.)
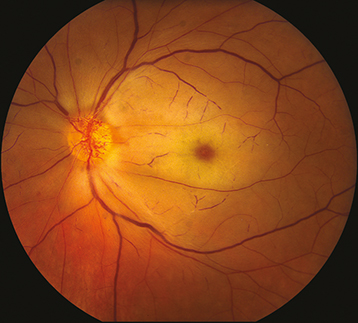
Figure 11.6.1: Central retinal artery occlusion.
Critical
Superficial opacification or whitening of the retina in the posterior pole and a cherry-red spot in the center of the macula (may be subtle).
Other
Marked RAPD. Narrowed retinal arterioles; boxcarring or segmentation of the blood column in the arterioles. Occasionally, retinal arteriolar emboli or cilioretinal artery sparing of the foveola is evident. If visual acuity is light perception or worse, strongly suspect ophthalmic artery occlusion.
CRAO is treated as an acute stroke and immediate referral to an emergency department with a stroke center is warranted. If GCA is suspected, see 10.17, Arteritic Ischemic Optic Neuropathy (Giant Cell Arteritis) for treatment recommendations.
For specific management of ocular signs and symptoms, there are anecdotal reports of improvement after the following treatments, if instituted within 90 to 120 minutes of the occlusive event. None of these treatments have been proven effective in randomized, controlled clinical trials and should not be considered standard of care.
Immediate ocular massage with ophthalmic contact lens (e.g., gonio lens, fundus contact lens) or digital massage.
Anterior chamber paracentesis: See Appendix 13, Anterior Chamber Paracentesis.
IOP reduction with acetazolamide, 500 mg i.v. or two 250-mg tablets p.o. or a topical beta-blocker (e.g., timolol or levobunolol, 0.5% daily or b.i.d.).
Thrombolysis.