Ocular irritation, burning, foreign body sensation, tearing, and redness of one or both eyes. Usually worse in the morning.
Critical
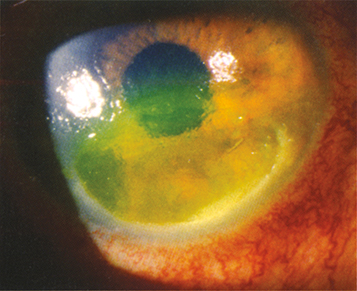
Inadequate blinking or closure of the eyelids, leading to corneal drying. Punctate epithelial defects are found in the lower one-third of the cornea or as a horizontal band in the region of the palpebral fissure (see Figure 4.5.1).
Figure 4.5.1: Exposure keratopathy stained with fluorescein.
Other
Conjunctival injection and chemosis, corneal erosion, infiltrate or ulcer, eyelid deformity, or abnormal eyelid closure.
Prevention is critical. All patients who are sedated or obtunded are at risk for exposure keratopathy and should receive lubrication according to the following recommendations.
In the presence of secondary corneal infection, see 4.12, Bacterial Keratitis.
Correct any underlying disorder.
Preservative-free artificial tears q2–6h. Punctal occlusion with plugs may also be considered.
Lubricating ointment q.h.s. to q2h.
Consider eyelid taping or patching q.h.s. to maintain the eyelids in the closed position. If severe, consider taping the lateral one-third of the eyelids closed (leaving the visual axis open) during the day. Taping is rarely definitive but may be tried when the underlying disorder is thought to be temporary.
A potential in-office procedure includes placement of self-retained amniotic membrane tissue (e.g., sterilized, dehydrated amniotic membrane covered by a bandage soft contact lens or frozen, specialized plastic ring–mounted amniotic membrane such as Prokera).
When maximal medical therapy fails to prevent progressive corneal deterioration, one of the following surgical procedures may be beneficial:
Partial tarsorrhaphy (eyelids sewn or glued together).
Eyelid reconstruction (e.g., for ectropion).
Eyelid gold or platinum weight implant (e.g., for seventh cranial nerve palsy).
Orbital decompression (e.g., for proptosis).
Conjunctival flap, sutured/glued amniotic membrane graft, or Descemet membrane graft (for severe corneal decompensation if the preceding fail).
Reevaluate every 1 to 2 days in the presence of corneal ulceration. Less frequent examinations (e.g., in weeks to months) are required for less severe corneal disease.