(See Figure 11.31.1.)
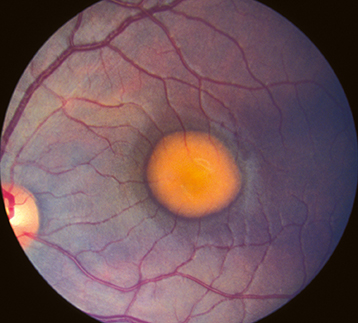
Yellow, round, subretinal lesion(s) likened to an egg yolk (lipofuscin) or in some cases to a pseudohypopyon. Typically bilateral and located in the fovea, measuring approximately one to two disc areas in size. Likely present at birth, though may not be detected until examination is performed. Ten percent of lesions are multiple and extrafoveal. ERG is typically normal, while EOG is abnormal, showing severe loss of the light response.
The lesions may degenerate, and patients may develop macular CNV (20% of patients), hemorrhage, and atrophic scarring. In the scar stage, it may be indistinguishable from AMD. Hyperopia is common due to shortened axial length along with angle-closure glaucoma; may also have esophoria or esotropia.
Inheritance
Autosomal dominant with variable penetrance and expression. Due to a mutation of the BEST1 gene. An autosomal recessive form with many small vitelliform lesions is also occasionally seen and diagnosed earlier in age than the autosomal dominant form.