


A.6. Describe the ventricular interaction in cardiac tamponade.
Answer:
RV and LV function are interdependent due to their shared septum and pericardial constraint, sometimes termed parallel ventricular interdependence. Under normal conditions, there is sufficient compliance in the cardiac chambers and pericardium to accommodate distension from diastolic filling of one ventricle with minimal effect on the function of the other. In cardiac tamponade, this shared septum impairs optimal diastolic filling with increasing pericardial constraint. Pericardial fluid competes with the cardiac chambers for a portion of a fixed cardiac volume. Increasing pericardial pressure increases filling pressures of all the cardiac chambers. Under these conditions, instead of free wall distension, RV filling during inspiration shifts the interventricular septum toward the left ventricle; this accommodates the diastolic volume augmented by negative pressure inspiration at the expense of LV cavity size and compliance (Figure 12.4).
Figure 12.4.: Parallel Ventricular Interdependence.
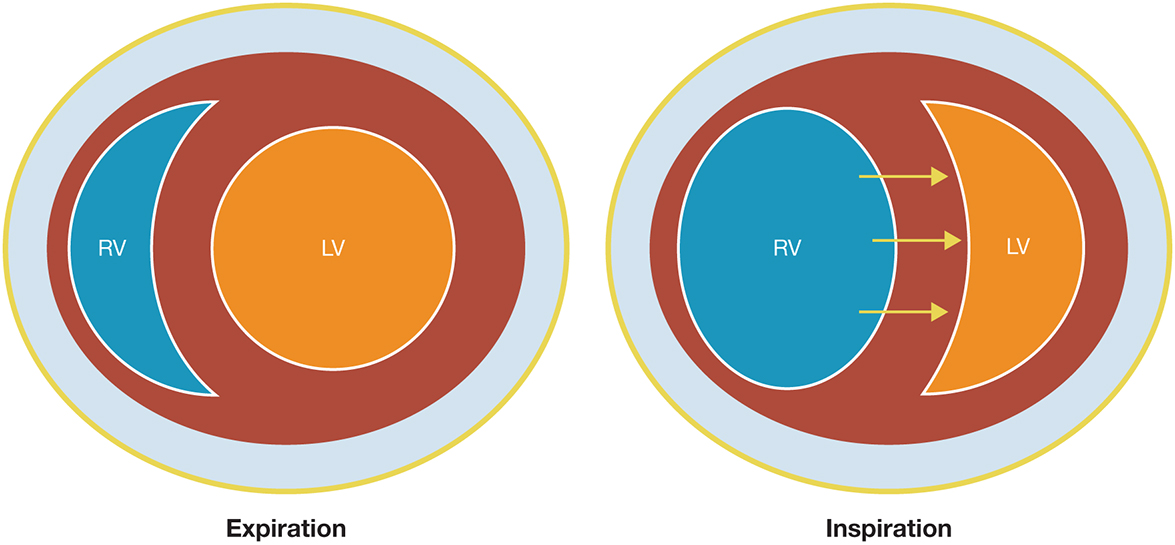
Parallel ventricular interdependence. In cardiac tamponade, diastolic ventricular filling is constrained by increased pericardial pressure. To accommodate increased right ventricular diastolic volume during inspiration, the interventricular septum shifts toward the left ventricle (LV). This alters LV compliance and mechanics, leading to a decrease in LV stroke volume during inspiration. RV, right ventricle.
Series ventricular interdependence refers to the dependence of LV filling on RV output. Changes in RV SV affect LV diastolic volume, albeit with a delay of several seconds as it crosses the pulmonary circulation to the left heart. This pulmonary transit time is highly variable, lasting 5 to 10 seconds in normal subjects at rest. In cardiac tamponade, the increasing dependence of RV filling on intrathoracic pressure results in similar phasic changes in pulmonary venous return and LV SV.
Taken together, cardiac tamponade exaggerates both parallel and series ventricular interdependence: to fill the right ventricle, LV filling and SV becomes compromised, and LV filling is reduced if RV SV is impaired. This augmented variability in ventricular filling can be measured with Doppler echocardiography of the transmitral and transtricuspid inflow velocities, demonstrating an increase while simultaneously reducing the other.
Depending on chronicity, size, and etiology of the cardiac tamponade (ie, fluid vs clot, regional vs global cardiac tamponade), exaggerated atrioventricular interdependence can develop as they become subject to worsening pericardial constraint and pressure. Normally, venous return to the atria is maximal during ventricular systole and early diastole (corresponding to the x-descent, v-wave, and y-descent). With cardiac tamponade, the atria fill more readily when the ventricles are small (ie, during ventricular systole) and passive atrioventricular filling becomes increasingly influenced by intrapericardial pressure as a Starling resistor. This leads to a deep x-descent as atrial filling occurs almost solely during ventricular systole and the loss of the early diastolic y-descent, both characteristic findings in cardiac tamponade (Figure 12.5). Eventually, pericardial pressure increases sharply as pericardial compliance is exhausted. This pressure first compresses the thin-walled atria, followed by the low-pressure RV, and finally the left ventricle.
Figure 12.5.: Central Venous Pressure (CVP) Waveform Abnormalities in Cardiac Tamponade.
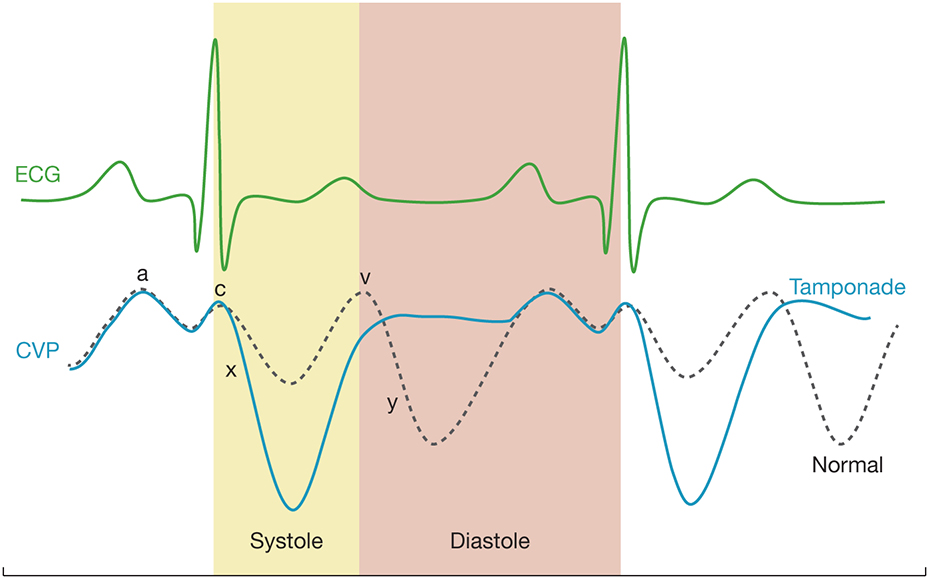
Central venous pressure (CVP) waveform abnormalities in cardiac tamponade. Compared with normal conditions, the CVP trace in cardiac tamponade is characterized by a deep x-descent, signaling increased atrial filling during ventricular systole (ie, when the ventricles are small) and a loss of the y-descent. The y-descent normally coincides with opening of the tricuspid and mitral valves. During this period of diastole, the atrium acts as a conduit between the large central veins and the ventricle with venous return following the hydrostatic pressure gradient to the ventricle. In cardiac tamponade, pericardial pressure acts as a Starling resistor to venous return on the atrium, dampening and eventually eliminating the y-descent as a result. ECG, electrocardiogram.
References
- Buckberg G, Hoffman JIE. Right ventricular architecture responsible for mechanical performance: unifying role of ventricular septum. J Thorac Cardiovasc Surg. 2014;148:3166.e4-3171.e4.
- Hamzaoui O, Monnet X, Teboul JL. Pulsus paradoxus. Eur Respir J. 2013;42:1696-1705.
- Hoit BD. Pathophysiology of the pericardium. Prog Cardiovasc Dis. 2017;59:341-348.
- Spodick DH. Pathophysiology of cardiac tamponade. Chest. 1998;113:1372-1378.