Objectives ⬇
- Distinguish among learning environments as simulations, virtual worlds, or games.
- Describe the role of simulation in nursing informatics education.
- Compare and contrast simulations, virtual worlds, and games as informatics tools for nursing education.
- Assess strategies for choosing among a simulation, virtual world, or game as the best choice for instructional delivery in a given educational situation.
- Explore the role of simulation, virtual worlds, and games in nursing education.
- Differentiate between using a live clinical information system or simulated electronic health records for educational purposes.
- Assess the realities of augmented reality and virtual reality in relation to nursing education currently and within the foreseeable future.
Key Terms ⬆ ⬇
Introduction ⬆ ⬇
The use of latex-based and virtual simulation (Figure 20-1), virtual worlds, and game mechanics in nursing education was increasing, but with the COVID-19 pandemic, their integration really escalated to meet the needs of students who could not attend clinical experiences or classes. Many schools and staff education departments have employed these techniques to provide efficient, effective, and engaging educational experiences for their students and staff. The schools and other educational entities began realizing the benefits of these educational modalities. The monumental National Council of State Boards of Nursing (NCSBN; Hayden et al., 2014) simulation study brought national attention to the need to enhance, extend, or replace clinical and practicum hours with other effective means, such as simulation. In this chapter, we will explore simulated documentation, simulation, virtual worlds, and game mechanics used in teaching nursing informatics competencies and nursing education.
Figure 20-1 Latex-Based Simulation

An illustration features a patient lying on a bed with an I V attached. A nurse checks the I V, and a doctor places a stethoscope on the patient's chest.
Even though there are many nursing students, nursing educators, and nurses using these technologies, no clear understanding of the terminology associated with these learning modalities exists. Therefore, it is important to define this terminology when discussing these technologies and their effect on nursing informatics and nursing education.
- Simulations are imitations of real-life events or circumstances; in nursing education, simulations are used to replicate a clinical scenario to provide an opportunity for practice in a mock situation. These simulations can be done with mannequins (latex-based simulation) or via role-play, web-based applications, or virtual simulation in a virtual world.
- A simulator is a mechanical or electronic device that provides an environment in which a simulation can occur.
- Simulated documentation refers to any simulated electronic format or electronic health record (EHR) that is accessed and used by the learner to actually document simulated nursing care for educational purposes.
- A simulation scenario is a situation or case developed in a simulation setting to mimic an actual practice situation.
- A game is a structured activity undertaken for enjoyment.
- In education, edutainment is the combination of education and entertainment to make learning fun.
- Game mechanics are the rules, instructions, directions, and constructs that the learner interacts with while playing the game. For educators, it is essential that any game mechanics they use be engaging and satisfying for the learner.
- Gameplay is how the learner interacts with or plays the game. This is extremely important to understand to be able to appreciate how the game functions and the learners function, play, and learn.
As you progress through the chapter, you will delve into simulated documentation, simulation, game mechanics, virtual worlds, and the realities.
Setting the Stage ⬆ ⬇
The use of game mechanics in educational, or serious, games and virtual world simulation continues to grow, with a great deal of research effort and funds directed toward the discoveries of their best uses. Educational games and virtual world simulations share some characteristics, and it is difficult to find a pure experience in any of the genres. Simulations may have gamelike qualities, and virtual worlds may be used to present a simulation.
Case Scenario
Joe sits down at the computer and logs in to StratWorld, a virtual world that enables users to create their own team and then compete against other teams created by other StratWorld players. The developers of StratWorld created interesting challenges, part intellectual and part brute force, which teams strive to solve before competing teams solve them first.
After Joe logs on, he is presented with a three-dimensional (3D) view of a forest. Directly in front of him is a 3D figure that looks very much like Joe, except for having broader shoulders, a more rugged face, and better skin complexion. This is Joe's avatar, his representation of himself in StratWorld. Joe can change his avatar's appearance as he wishes, but he likes to stick to something close to what he actually looks like. All the members of one of his opposing teams in StratWorld prefer to appear as masses of glowing tubes, but Joe thinks they are strange.
Today, he is recruiting for his virtual team, so he ducks into his inventory (i.e., a place to store items his avatar can wear and use) and dons his manager's jacket. “Joe's Team” is proudly displayed on the back. Joe is proud of the jacket; he created the lettering himself in a graphics program, uploaded it to StratWorld, and then added it to a plain jacket and gave a copy to all new members of his team. As in many virtual worlds, clothes do make the man, woman, or thing.
Using the arrow keys and the mouse to manipulate his avatar, Joe begins to make his avatar walk down the forest trail. He is looking to recruit an ogre for his team to beef up its physical offensive capabilities and replace the recent loss of Charlie the unicorn. Ogres are big and strong, perfect for the task. Joe is a little nervous because he has never been to this part of StratWorld before and explorations in new areas can be fraught with peril. After a brief sojourn, Joe comes upon an ogre sitting in a daisy-strewn clearing, picking its teeth with a small sapling ripped from the ground. “Ogre!” Joe shouts. “I need someone to smash through things for my team. Interested?”
“What's in it for me?” the ogre asks, thumping its chest with the remains of the sorry sapling and splintering it into oblivion. “Darn! That was a good toothpick!” The chirping of birds and the droning of insects in the foliage, all part of the normal background noise here, suddenly stop. Joe picks up on this environmental clue and, just as in the real world when this happens, knows he is in danger.
Joe ponders the question. He knows he is talking to a nonplayer character (NPC), one that seems to have a brain behind the 3D facade but that in reality has very clever programming attached to it so that it can seem to carry on an intelligent conversation. Some companies call this artificial intelligence, but both the creators of these environments and the scholars who study them hotly debate the proper use of that term. Joe also knows that the world is constructed so that he has to balance his profits from game wins with overhead costs, such as players' salaries and equipment maintenance. He needs to make an offer to the ogre. An offer of too little would insult the ogre, and a fight between it and Joe would be the probable result. Joe's avatar could die, an inconvenience that would cost him time and loss of reputation with other StratWorlders. A generous offer would probably be accepted but might bankrupt Joe over time. Joe needs to balance his needs and costs and think outside the box. It is a complex problem-solving situation!
“Okay, Ogre, here's the deal. Pay is $900 a month, and . . .” Joe attempts to continue, but the ogre quickly rises in an aggressive manner. “Wait! Let me continue! I know that's a little less than normal, but I'll throw in a nice, new sapling each week for tooth maintenance! How about it?”
The ogre sits back down and eyes Joe warily. “Just need to pick tooths, not maintain ants. Contract for . . .” (the ogre pauses to quickly count its fingers) “10 months?”
“Sure, sure, but if you are injured, you go to half pay until you can play again,” Joe answers.
“I still get toothpick each week, even if hurt?”
“Absolutely. I mean, yes.”
The ogre leans forward on its haunches. “Sound good! You go. I follow.”
“One more thing, Ogre. What do I call you?” Joe asks.
“Daisy! You managers sure are stupid!”
Joe takes Daisy back to his office by teleporting there, which is a way to move from one place to another with a simple click of a button. Joe pulls up a map of StratWorld, locates the land he owns, and clicks on it for instantaneous transport. Joe sends Daisy the ogre to practice smashing down walls in his training field and then pauses for a moment to admire his recreation of his grandfather's old rolltop desk. He recreated it from an old photograph just for his office in StratWorld. Looking out the window, he sees Daisy running out on the training field. He sits down at his desk to go over his team's statistics. With the addition of Daisy to the team, Joe needs to recalculate all his strategies. He must determine how he can acquire a sapling each week for Daisy. Where will he get one, and how much will it cost? Then he needs to send out an acceptance to a recent invitation from the game developers to participate in next week's challenge. A win would be sweet, but it will be a busy week of preparation!
Before Joe hunkers down to work, he sends an instant message to Kathy, an admirable opponent in StratWorld against whom he has competed several times. Typing furiously and with a certain glee, he writes, “Hi, Kathy, guess what? I'm gonna DUST your team in the next challenge!” Kathy's reply is swift: “Bring it on, Joe, bring it on!”
Case Scenario Discussion
This is a brief description of what occurs in many online virtual environments today. People create a presence in the environment and then manipulate events for a desired outcome. They explore, build things, interact with others, and try to achieve goals. The story is fictional; there is no StratWorld, but games do exist for which people build teams and compete against one another. So is StratWorld a simulation, a virtual world, or a game? What do you think? Think about simulations you have experienced or heard of, games you have played, and anything you have read about virtual worlds. Try looking up some definitions online. Write down your thoughts, and come up with some justifications that back your decision.
Note that avatar realism continues to improve; some are so humanlike that they are referred to as virtual humans (Stuart, 2018).
Examples of Simulation in Nursing Informatics Education ⬆ ⬇
Following are two examples of using simulation in nursing informatics education. In the first example, the EHR is part of a larger simulation scenario that mimics a real-life clinical case, and in the second example, the EHR itself functions as a simulator and becomes a true-to-life learning tool.
In the first example, the patient call bell is ringing; you enter the room to find the patient verbalizing complaints of chest tightness. In a moment, the patient becomes unresponsive, and a code is called. The team quickly responds, initiating resuscitation measures per the advanced cardiac life support protocol. You review the EHRs with the attending physician while discussing your assessment before the code. After a short while, the resuscitation efforts are successful, and the patient is stable enough for transfer to the intensive care unit. You complete your documentation in the patient's EHR, the simulation scenario ends, and the debriefing begins. The instructor provides feedback not only on actions taken within the simulation scenario but also on the use of the EHR as an important resource for patient information and documentation.
In the second example, it is the first day of a new course, and rather than a lecture-based class with an accompanying textbook, the instructor uses an active learning approach with case studies delivered through an EHR interface to facilitate the learning and application of clinical concepts. In this example, rather than being part of an entire simulation scenario, the EHR itself is the learning tool providing learners with a hands-on learning opportunity centered on accessing and using the information contained within the patient record. Choi et al. (2016) concluded that academic electronic medical records (AEMRs) would improve students' understanding of clinical practice: “[T]he findings of this study will provide important developments by applying an AEMR, which will augment students' informatics competencies and critical thinking, into the nursing curricula to better prepare the future workforce” (p. 264).
| Applications in Education to Enhance Learning |
|---|
| You are learning about informatics. What role or roles would the nurse informaticist assume in relation to each of these strategies? Reflect on nursing informatics' effect on each of the following instructional technologies and educational strategies described. |
| Massive Open Online Course |
|---|
| A massive open online course (MOOC) is a virtual or an online course with unlimited participation and open access via the web. The course runs over a set number of weeks using materials and resources available online. Some MOOCs have had up to 150,000 learners enroll, but most learners will not stay to complete the course. Murray (2019) reported “an astronomical dropout rate of about 96 percent on average” (para. 2). Traditionally, MOOCs are free and typically provide interactive opportunities using social media or other tools to support community interactions among learners and teachers. Learners select the courses they want to take and are in control since they set their own pace and attend or quit when they want. These factors place the responsibility of learning on the learner. “Much of the early enthusiasm for massive open online courses, or Moocs, focused on how they could disrupt and democratise education” (Murray, 2019, para. 1). |
| Reusable Learning Object |
|---|
| A reusable learning object (RLO) is an approach to content development, consisting of independent, self-contained, digital, multimedia e-learning resources, that breaks the content into chunks so that each object can be swapped, interchanged, substituted, and exchanged as needed, based on the characteristics of the learners and their specific learning needs. Typically, RLOs contain a presentation, an activity, links and resources, and a self-assessment. They are based on the object-oriented model from computer science; this paradigm intends to assimilate the advantages of modules and seeks to recycle these objects as needed.
RLOs can be used repeatedly in a variety of learning episodes. Each RLO has its own learning objective and can stand alone, but when many RLOs are strategically combined, a comprehensive learning experience can be crafted. To facilitate the ability to plug and play, RLOs must be easily adaptable, interoperable with the infrastructure, and organized using targeted metadata so that they can readily be extracted for reuse. RLOs are little chunks of learning that provide the right amount of information needed to assist the learner in meeting a specific learning objective.
|
| Multimedia Educational Resource for Learning and Online Teaching |
|---|
| Multimedia Educational Resource for Learning and Online Teaching (MERLOT) (www.merlot.org/merlot) is a web-based open resource that “provides access to curated online learning and support materials and content creation tools led by an international community of educators, learners, and researchers.” It also includes an information technology community portal (www.merlot.org/merlot/InformationTechnology.htm). |
| Adaptive Learning |
|---|
| Adaptive learning is an educational strategy that manipulates how the learning environment is displayed to the learner to allocate and mediate the learning resources, based on each learner's unique learning needs. The adaptive behaviors and activities are based on mathematical paradigms of knowledge and use artificial intelligence (AI) in an approach to actively tailor content to meet each learner's needs by adapting to the knowledge of the learner. This is a learner-centered approach because the learner's needs drive which educational episodes they are afforded.
|
Nursing Informatics Competencies in Nursing Education ⬆ ⬇
In the late 1990s, researchers identified that healthcare professionals needed to possess both skills in and knowledge of informatics (American Association of Colleges of Nursing, 1999; Gassert, 1998; Pew Health Professions Commission, 1998). In addition, information technology was identified as a key measure in improving patient safety and quality of care (American Academy of Nursing, 2003; Institute of Medicine, 2000). In response to the increasing demand for practitioners to become skilled in this area, coupled with the absence of research-based informatics competencies, a Delphi study was used to identify informatics competencies for nurses at four levels of practice (Staggers et al., 2002). In essence, this seminal study created informatics competencies for entry-level nurses through informatics specialists and innovators, with a focus on computer skills, informatics knowledge, and informatics skills.
Although informatics competencies for nurses have been identified, the degree to which schools of nursing have woven them into the curriculum varies greatly (Carty & Ong, 2006). In a study conducted by Fetter (2009), a survey of graduating senior nursing students ranked the following competencies with which they had no experience or minimal skill: (1) using applications to document, (2) creating an electronic care plan, (3) valuing informatics knowledge for practice, (4) valuing informatics knowledge for skill development, and (5) using applications for data entry. Hunter et al. (2013) developed an online self-assessment tool, the TIGER-Based Assessment of Nursing Informatics Competencies (TANIC); this instrument assesses the Level 1 Beginning Nurse and Level 2 Experienced Nurse competencies. McGonigle et al. (2013) developed the Nursing Informatics Competency Assessment (NICA) for Level 3 Informatics Nurse Specialist and Level 4 Informatics Innovator, based on the seminal work of Staggers, the current literature, and expert input. This online self-assessment was noted in the 2014 American Nurses Association Nursing Informatics: Scope and Standards of Practice, Second Edition. These self-assessment tools are discussed in Chapter 7, Nursing Informatics as a Specialty.
The question then becomes, Which best practices will ensure that students become prepared in informatics? The National League for Nursing (2015) realized the need to prepare students for the technology-rich healthcare environments. Nursing educators and administrators indicated the need to make sure that informatics is integrated throughout the curriculum and that experience with nursing informatics is provided during clinical rotations as well. Little clinically related informatics content and few such learning experiences were provided in nursing programs. Technology tools containing care planning software and clinical information systems were least likely to be incorporated into the courses, and the lack of these tools continues to be an issue. Another area of concern is the preparation of the nursing informatics faculty in the use of these tools. Rajalahti et al. (2014) made several recommendations about competencies, including the following: “A description of nursing informatics competencies for nurse educators is needed at a national and global level. Advanced nursing informatics programmes are needed in the nurse educators' training programme” (p. 64). Nursing faculty must be prepared to use these technologies. With emerging technologies in nursing and healthcare education, the use of these technologies, including simulation, to allow students to use informatics in an active manner and in an authentic and realistic learning context is one potential approach to remedying these shortcomings.
A Case for Simulation in Nursing Informatics Education and Nursing Education ⬆ ⬇
A simulation recreates a real-life set of conditions or events with as much fidelity as possible (Alessi, 1988). Aldrich (2010) contended that simulations develop cognition (i.e., learning-to-know skills), ethics and roles (i.e., learning-to-be skills), and application capabilities (i.e., learning-to-do skills). Unlike games, however, simulations are not necessarily designed to be fun.
Simulations contain four major components: prebrief, enactment, debrief, and assessment (PEDA) (refer to Table 20-1). Every simulation should have these elements in order to prepare and assess students while also facilitating learning through doing and reflection. The most important translational PEDA components are the prebrief and debrief. It is imperative that learners know exactly what is expected and be prepared for the enactment in the prebriefing. When done well, debriefing helps learners reflect on the authentic experience and solidifies the learning by facilitating the transfer of theory and skills to their real practice setting. Graduate nursing education is an area that is expanding learners' simulated learning episodes. Woroch et al. (2018) described a drug-seeking telephone triage scenario simulation in which family nurse practitioner (FNP) students collaborated with psychiatric mental health nurse practitioner students. Robinson-Reilly et al. (2020) stated that “[s]imulated telehealth allows students to engage in a learning environment that closely reflects real-life experiences without posing a threat to either the student or the patient” (p. 49). Harris (2020) simulated lacerations, abscesses, and suspicious lesions with nurse practitioner students. Harris et al. (2016) believed that simulation could assist FNP students with their role transition from generalist to advanced practice by doing the following:
Table 20-1 Simulation PEDAEach simulation must have four components: - Prebrief
- Enactment
- Debrief
- Assessment
|
Prebrief | Students receive the simulation information, the goal, the educational outcomes, and the related course or program outcomes. The simulation should be explained and focused for students. They should know how to prepare for the activity and be told what is expected, provided with the background necessary to be able to fully enact their role in the activity, and given the specifics about how they will be assessed. They must also be provided with the time frame within which the simulation must be completed. |
Enactment | The simulation area is prepared to facilitate the activity. Students enact the role assigned and complete their assigned activities during the established time frame. |
Debrief | Debriefing is “a student-centered discussion during which the participants and observers reflect on performance during the scenario and make recommendations for future practice” (Mastrian et al., 2011, p. 351). The debriefing can be done one-on-one or with entire teams. Faculty can help students during and after their activities by focusing on breakdowns and areas of growth to hone future learning episodes (Tanner, 2006). Following the completion of each activity, it is important to do the following: - Answer students' questions.
- Address students' perspectives, perceptions, and concerns.
- Emphasize and reinforce specific learning outcomes.
- Create authentic linkages to the real world.
- Assess students' learning. What did they learn?
- Validate what students learned.
Ask the students to reflect on the simulation activity, both how they felt during the activity and how they feel now that the activity is completed. - What did students enjoy the most and the least about the activity?
- What were students' perceptions regarding the activity?
- Can students describe the emotions they experienced while completing the activity?
- How do students describe the interpersonal interactions or the enactment of their role?
- What were the major points of the activity?
- Did students experience any problems that affected their ability to make the necessary decisions during the activity?
- How could you prevent these problems in the real world?
- If you could not prevent them, how could you avoid them in the real world?
- What did students learn?
- What did students learn that was new to them?
- Did things that students already know take on new meanings after the activity?
- Was there a specific aspect of the activity where students learned the most?
- Reflect on students' perceived learning and validate what they learned.
- Would students recommend any changes to enhance the activity? If yes, what changes, and how would each change enhance the activity?
- What will students take with them after having completed this activity?
|
Assessment | Students should be provided with a detailed explanation of how they will be assessed and graded, which relates to the goal; educational outcomes; and, if applicable, course or program outcomes. Detailed rubrics are recommended. The assessment process must be shared during the prebriefing. If the activity is not being graded, a self-assessment should be provided for students so that they know how to evaluate their own performance. |
Developed by Dee McGonigle.
- “Allowing FNP students opportunities to gain confidence in a risk-free environment.
- Providing FNP students an entire comprehensive office-based or acute patient care experience.
- Reinforcing classroom content and bridging the theory to practice gap” (p. 14).
Simulations may be experiential and task based, in which the learner takes on a first-person role and executes a self-chosen series of decisions by manipulating the variables in the simulation toward a desired outcome (Aebersold & Tschannen, 2013; Gredler, 1996). Simulations may also be symbolic scenarios in which the learner directly manipulates variables, sees the results of changes, and then makes decisions on how to continue in the simulation. Spreadsheets are often used for this type of simulation. Symbolic simulations are good choices for discovering principles, misconceptions, and relationships and for fostering understanding, prediction, and solution development (Mastrian et al., 2011).
Simulations may use a process known as scaffolding (Jonassen, 1999; Podolefsky et al., 2013) to assist in acquiring the accepted level of proficiency. An example of scaffolding is when corrective feedback is initially used to correct user mistakes and ensure success and then the feedback fades away when it is no longer needed.
Medical simulations use realistic three-dimensional computer models of humans to investigate new medical possibilities and test assumptions (i.e., learning-to-know skills). Simulations of drawing blood and performing complex medical operations are used to teach learning-to-do skills.
In general terms, a simulator can perhaps best be described as a tool designed to emulate some aspect of the clinical practice environment, which may be focused on a single task or designed to mimic a complete patient care situation (Gaba & DeAnda, 1998). At its essence, it is any device that is used to create a realistic learning experience for the learner but that removes the risk associated with learning during hands-on patient care. A simulator offers the unique ability to create a realistic learning environment that is safe, structured, and supportive for the learner (Bligh & Bleakley, 2006).
Simulators encompass a broad range of devices, such as partial task trainers (e.g., an IV insertion arm); screen-based simulations, including simulated EHRs, documentation, and environments that replicate a realistic patient-care area (virtual simulation); and complex computer-driven human-patient simulation mannequins (i.e., latex-based simulation). Web-based virtual standardized patients are also increasing in use. It is important to understand which of these products you are using, one in which you enter and interact in a virtual world, access a web-based product, or interact in a latex-based lab. Although each of these simulation modalities can be used alone, they can be powerful learning tools when used together to create a realistic patient care scenario. When designing simulation learning environments, “[i]nnovative educators design learning environments that encourage active engagement in the learning process. . . . Active engagement creates a personal connection with the learning experience and motivates the learner to take greater responsibility in the learning process” (Fisher, 2016, p. 9). According to Gaba (2004), the goal of simulation is a seamless immersion into the simulated practice environment during which learners are drawn into the reality of the environment or task at hand. Hertel and Millis (2002) noted that this is a cooperative process whereby learners come together in an authentic setting and begin to learn from one another. Darragh et al. (2016) recommended realistic scenarios that elicit autonomous problem-solving and decision-making to immerse and engage the participants in active learning and critical thinking (Figure 20-2).
Figure 20-2 Simulation Can Bridge the Gap
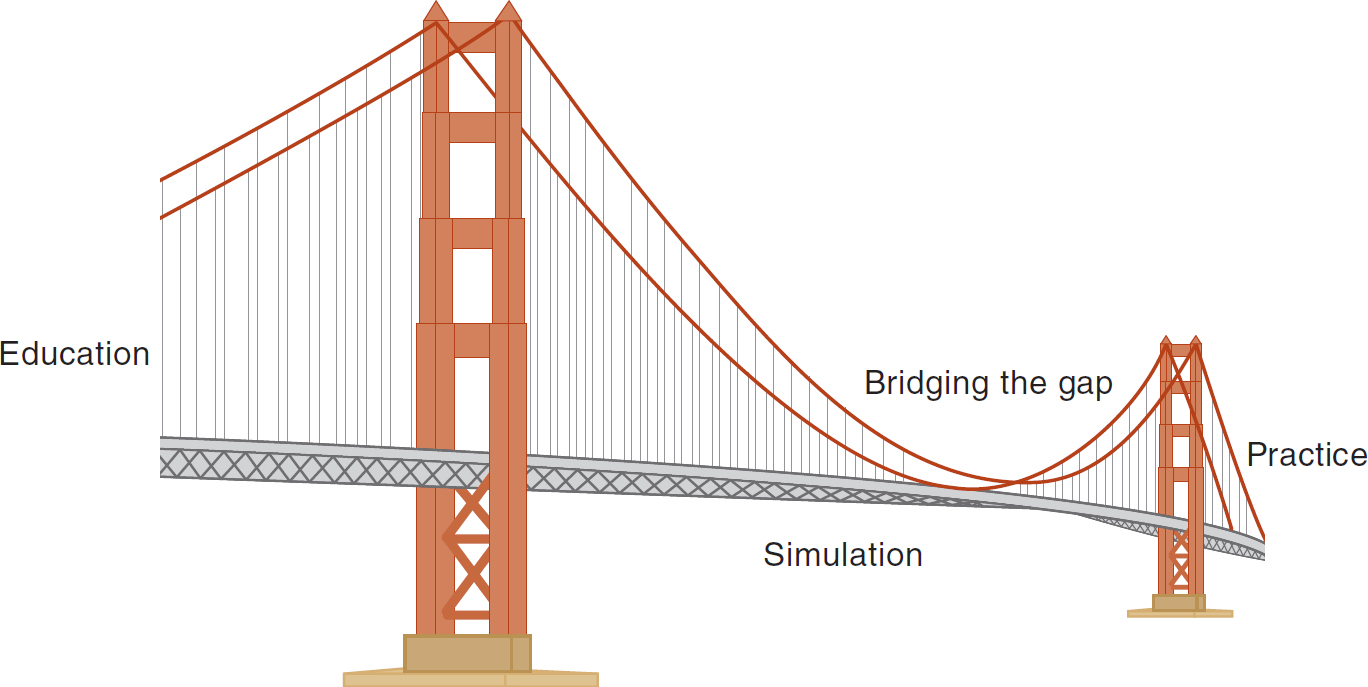
An illustration depicts a suspended cable bridge linking two columns; one column represents education, and the other signifies practice. The simulation bridges the gap between the two columns.
Considering the realistic nature of simulation and its hands-on active approach to learning, it seems that the use of simulation modalities can be a powerful tool in moving student nurses-indeed, any practitioners-toward achieving the informatics competencies. Recall the examples given at the beginning of this chapter. In both examples, simulation is used to incorporate nursing informatics into the context of patient care, thereby giving students an authentic learning experience that can be applied in clinical practice.
According to the NCSBN national simulation study (Hayden et al., 2014), 50% simulation can be effectively used in various program types, in different geographic areas, and in urban and rural settings with good educational outcomes. The NCSBN study results and the lack of available quality clinical and practicum placements are prompting the move to integrate more simulation into nursing education. Virtual and latex-based simulations are valuable educational assets at all levels of nursing education. They provide a safe, authentic environment in which to develop knowledge, skills, and attitudes before interacting with actual patients. There is no risk to patients, and students can practice and receive assessment and feedback for controlled episodes, including unusual events. Simulation relates well to adaptive learning methods, such as branching logic, that allow the learner to guide the learning. The nurse educator can tailor the simulation to the learning needs of the students and provide deliberate practice with feedback. The learner can learn, relearn, and hone skills while safely practicing in dynamic and complex situations with a view to decreasing and eliminating mistakes.
Incorporating EHRs Into the Learning Environment ⬆ ⬇
There are two main approaches to the incorporation of an EHR into the learning environment, whether used within a simulated clinical environment as part of a patient care scenario or as a stand-alone learning tool. First, the EHR can be created specifically for simulation purposes; options range from a well-developed Microsoft Access database to commercially available products designed specifically for simulation purposes. Second, the simulation may use a real EHR system either within a hospital-based simulation center or through a partnership with a healthcare facility or an EHR vendor. Raths (2020) found that many health centers are using commercial EHRs.
There are certain advantages and disadvantages to each simulated documentation solution (Figure 20-3). Live documentation systems provide learners with a realistic experience and can be incorporated into the learning environment, but they also present certain drawbacks: (1) They are designed for the patient care environment, not the learning environment, and therefore lack an efficient feedback mechanism for learners; (2) they are designed to work in real time, not simulated time, which creates issues with data recall, especially when a record may be used repeatedly over a period of months or years; and (3) if a system is overly complex, it may unintentionally focus the learning on the specific system rather than on the process of data retrieval and documentation. Refer to Research Brief 1 for more on the challenges of teaching clinical documentation skills in an EHR.
Figure 20-3 Simulated Documentation Nurse/Patient. You are working as a team. This is Mr. Poli, and as your simulated patient, you will be saving him from falling when you assist him to the restroom and determining why he is unsteady. At the end of your shift, you will document the nursing care you provided to this patient. When you leave, Mr. Poli will tweet about his experience with each of you as his nurse and post comments about the care you provided. It is important to simulate not only what the nurse must document but also what the patients document and how they use social media to describe their care experience. It is important that you realize that patients take note of your actions and use social media to share their opinions and observations. Think about your best and worst experiences in health care. They might be something you experienced yourself or with a loved one. Where and what would you share through social media?

A healthcare practitioner observes a monitor that depicts a three-dimensional simulated healthcare scenario. In the simulation, a patient is portrayed standing at a hospital reception area.
One system designed specifically for simulation is the web-based medical chart (WMC). This system requires four components: (1) a database, (2) dynamic web page shells, (3) a server, and (4) computers with access to the internet. With this system, a Microsoft Access database is created to hold administrative information about the simulation scenario and other pertinent overview information accessible by only the instructor and the simulated patient data, simulated patient documentation, student documentation entries, and learner feedback from instructors. Each time a learner logs in to the WMC system via the internet, the server custom creates the requested page using the existing database information, user-specific information, and web page shells to create a realistic EHR for use by the student. Although this type of system offers a great deal of flexibility because it is custom created by the end user (and is certainly a cost-effective solution), it requires that the simulation instructor have a strong background in computer science and information technology to create and maintain the database and supporting materials.
| Research Brief 1 |
|---|
| Faculty perceptions of the challenges of teaching undergraduate students proper clinical documentation in both paper-based and electronic systems are described in a qualitative research study by Mahon et al. (2010). In this study, participants (N = 25) were interviewed using both open- and closed-ended questions, and results were analyzed using a constant comparative method. The most common method of teaching documentation skills was some variation of the demonstration-return-demonstration method. Faculty members were concerned about the amount of time it took to hone documentation skills in the actual clinical area, indicating that a median of 2 hours of an 8-hour clinical day were consumed by this task, and shared that there was seemingly little documentation taught in the classroom or laboratory. Faculty relied heavily on experts in the clinical setting and used their documentation as models for students to emulate. In the case of the EHR documentation, on-site nursing experts proficient in the use of the system were especially useful as role models. However, faculty remained concerned that using the electronic system and the endless drop-down menus might actually interfere with the development of nursing expertise and critical thinking.
One crucial issue that was shared by faculty regarding electronic documentation was that the clinical facility provided the instructor with only one access code so that all the students in the clinical group used the same code to document and there was limited access to computers on the clinical unit. The faculty was very concerned about the legal and ethical issues for appropriate documentation and the provision of care, such as on-time medication administration in a group of 8 to 10 students with one access code.
The authors suggested the need to integrate information competencies throughout the curricula and provide opportunities for faculty development in informatics. They suggested that “faculty competencies in the area of informatics must be identified and standardized” and faculty must learn to “model self-efficacy: the patience, support and persistence that characterize individual development within a professional discipline” (p. 620).
The full article appears in: Mahon, P. Y., Nickitas, D. M., & Nokes, K. M. (2010). Faculty perceptions of student documentation skills during the transition from paper-based to electronic health records systems. Journal of Nursing Education, 49(11), 615-621. https://doi.org/10.3928/01484834-20100524-06.
A qualitative research study by Kennedy et al. (2009) described the experiences and development of nursing process skills in nursing students (N = 5) using the Simulated E-hEalth Delivery System (SEEDS) learning innovation. In the SEEDS learning innovation, students were given written case studies and asked to enter the patient data in a simulated EHR and generate a care plan for the patient and family. The authors concluded that “[t]he technology provided an interactive venue for developing nursing process skills by linking assessment data from case studies with foundational concepts in nursing. . . . The exercise was authentic, dynamic, and learner centered” (p. 99). As a result of the themes discovered in this qualitative study, the authors proposed two hypotheses for future research to explore learning outcomes resulting from the use of a simulated e-health system:
Interaction is greater among technologically competent students who use electronic documentation for patient data during clinical conferences. These students interact more freely with other students and their faculty members and experience enhanced learner satisfaction. These students also demonstrate superior nursing process skills compared to students using traditional post clinical group discussion about patient care.
Technologically competent students also have higher test scores on specific topics compared to students who use paper-and-pencil means to organize the assessment data and develop care plans.
The full article appears in: Kennedy, D., Pallikkathayil, L., & Warren, J. J. (2009). Using a modified electronic health record to develop nursing process skills. Journal of Nursing Education, 48(2), 96-100. https://doi.org/10.3928/01484834-20090201-07.
|
Debriefing a simulation scenario is enhanced when a fully functional EHR is included. The EHR is linked to the simulation scenario and contains all the pertinent patient information for learners to access before or during the simulation scenario. It is imperative that the system incorporate the ability for learners to document just as they would in an actual clinical setting, with the capability of submitting the documentation to the instructor for evaluation and feedback. Being able to do this helps students feel practice ready. A major strength of this type of system is that it is a prepackaged, web-based solution that does not need to be created from scratch. Vanderbilt University Medical Center went with Epic. According to Raths (2020), “A decade ago, many academic medical centers built homegrown EHRs based on the innovative work of their own informaticians. Now, by and large, those same health centers use commercial EHRs from Epic or Cerner” (para. 1). Vanderbilt wants to guarantee that students, faculty, and clinicians can access data, investigate and test innovations, and assess the results.
In addition, many learning systems designed for simulation contain all the necessary tools for the instructor or simulation center staff to build the simulation scenario, including but not limited to programming guides, staging and scripting information for the scenario, and debriefing guides. Two potential disadvantages with any commercially available solution, however, are the cost to purchase it, which varies depending on the product and vendor, and the ability for or cost associated with customization.
Although the main disadvantages of a live system were discussed at the beginning of this section, the use of a real EHR system clearly provides learners with a truly authentic experience. One innovative solution to bridge this gap was developed out of an academic-business partnership between the Cerner Corporation and the University of Kansas School of Nursing. The SEEDS incorporated the use of Cerner Corporation's clinical information system and PowerChart application (Connors et al., 2002). This system was specifically adapted for educational purposes to address the learner's informatics needs. Similar to the WMC system, discussed previously, instructors developed the patient data stored within the Cerner Corporation's clinical information system database to create virtual patients within the system. Students could navigate through the system to view pertinent patient data and then document assessment information and create a plan of care within the PowerChart application. In addition, the instructor could access student documentation for evaluation and feedback. The SEEDS marked the first time a clinical information system was used in a simulated way for teaching curriculum content to health professional students (Kennedy et al., 2009). Refer to Research Brief 1 for a discussion of a study on the use of the SEEDS approach.
Challenges and Opportunities ⬆ ⬇
The adoption and use of simulation technologies present unique advantages and disadvantages. Using simulated medical records, either as a stand-alone learning tool or in conjunction with a complete simulation scenario, provides the learner with an opportunity for a realistic, hands-on learning experience. Major considerations when looking to adopt a simulated EHR include (1) cost, (2) ease of use for the instructor and learner, (3) technical support from the vendor, (4) time to build or develop the patient database, (5) additional simulation materials included with the package, (6) flexibility of the system to be customized and used as a stand-alone tool or in the setting of a full-scale simulation scenario, and (7) overall fidelity (i.e., realism).
In 2006, a coalition consisting of experts from the fields of health care, informatics, business and industry, and nursing proposed the Technology Informatics Guiding Education Reform (TIGER) initiative (Healthcare Information and Management Systems Society [HIMSS], n.d.). The aim of this group is to advance the integration of informatics core competencies into nursing education to provide better and safer care to patients. Of particular interest is the call to take an active role in the design and integration of informatics tools that are intuitive, affordable, usable, responsive, and evidence based (HIMSS, n.d.). This approach promotes truly new and innovative strategies for informatics education and creates significant opportunities for collaboration among industry, academia, and clinical practice.
The Future of Simulation in Nursing Informatics Education ⬆ ⬇
Simulation will clearly play an important role in the development of informatics competencies for student nurses and practitioners. One theme of simulation-based learning is practicing just as a nurse would in the actual clinical setting. Regarding facilitating the growth of informatics competencies, it is no different. If there are expectations regarding the use of clinical information systems and EHRs in the clinical setting, then the opportunity also exists for the incorporation of such tools into the classroom and simulated clinical setting.
Aside from using the simulated EHR in the setting of a clinical simulation scenario, opportunities also exist to incorporate the simulated EHR into the classroom in new and innovative ways. As mentioned at the beginning of the chapter in the second simulation example, the EHR can be used as an active learning tool within the classroom. Rather than requiring students to absorb information from a book, the EHR can become a powerful way for learners to make important connections about caring for patients with a specific disease process or to learn concepts of pathophysiology or pharmacology.
Game Mechanics and Educational, or Serious, Games ⬆ ⬇
Game mechanics are, simply put, the rules and limitations in which a game takes place. It is imperative that the rules be clearly stated in the instructions so that the players know what is expected of them and what the rules are that the game itself must follow. The mechanics determine how the players interact with the rules and the game responds to the players' moves or behaviors within the game, thus connecting the players' actions to the purpose of the game. People voluntarily play games because they are fun and embody many motivational aspects (Mastrian et al., 2011). Great games provide an optimally challenging state between boredom and frustration (Csikszentmihalyi, 1990). Games exist within a set of rules (Kelley, 1988; Salen & Zimmerman, 2003), and players receive feedback from their interactions in the game and rule space. According to Chen (2012), the rule space model facilitates the cognitive assessment and breakdown of a learner's skill and provides an understanding of the learning topics or concepts that are weaknesses or strengths for each learner.
Educational, or Serious, Games
Educational games are created intentionally for learning and fun, or edutainment; these games are referred to as serious games. They are a melding of educational content, learning principles, and computer games (Prensky, 2001) that should emphasize the value of the experience (Nemerow, 1996). Mungai et al. (2002) stated that the flow of an educational game may be under the designer's control more than that in a noneducational game and that feedback should be used to stress competency, not just achievement. The trick in designing an educational game is to maintain the same fun state found in noneducational games (Koster, 2004). “Contemporary teachers wishing to incorporate game-based learning whether doing so within a virtual environment, through video games, or by leveraging mobile apps and other technologies are at the forefront of a paradigm shift” (Bauman, 2016, p. 110).
Many types of games exist, and each type has a different potential for educational use (Mastrian et al., 2011). To learn to respond quickly and hone reflexes, action games may be used. Adventure games may be used to discover the unknown, such as diagnosing a patient's illness. Construction and building games could be used for building complex mental constructs that can be understood only through knowledge of their constituent parts and the ways in which they interrelate. Strategy games are great for nursing education teaching moments where careful, up-front planning is critical and on-the-fly adjustments to one's plan may be needed to ensure its success.
In role-playing games, the player takes on the role of one or more characters and improves the character while progressing through a storyline. Today, massive multiplayer online role-playing games are very popular; they use the internet to provide a shared, simultaneous experience for dozens or even hundreds of players. Role-playing games are an excellent way for nurse educators to guide students through any situation where a sequenced step-by-step introduction to the parts of the job or skill is required.
Casual games, also known as mini-games, are fairly new. These games are designed to be played in a short time span or for a few minutes a day over several days, weeks, or even months. Many online, browser-based games fit this category. Casual games may be useful for continuous reinforcement of basic concepts, emulating a slowly changing environment, and modifying the players' attitudes on a given topic over a period of time. To date, these games remain largely untapped as educational tools.
There are also gaming simulations. A simulation game uses game mechanics to imitate real-life activities in the form of a game. Refer to Research Brief 2 for a mixed-methods, quantitative and qualitative, study on the health and safety of home healthcare professionals, including nurses.
| Research Brief 2 |
|---|
| Darragh et al. (2016) stated that the rapid increase in home healthcare services is driving a need for additional trained home healthcare professionals. The training must be effective for managing personal health and safety hazards encountered when providing healthcare services in the home environment. The process of developing and evaluating an interactive virtual simulation training system to educate home healthcare professionals, including nurses, was described.
Sixty-eight home healthcare professionals participated in the study, with the majority being white (71%) and female (95%), with an average age of 49 years (with a standard deviation of 11.8 years). Sixty-seven percent worked in Ohio and Kentucky. The participants represented registered nurses, aides, homemakers, administrators, educators, occupational therapists, and physical therapists.
A mixed-methods design, qualitative and quantitative, using an interdisciplinary, participatory design methodology was used to develop a virtual simulation system to train home healthcare professionals to identify and manage health and safety hazards in the home using a gaming simulation learning approach. The participants identified the layout and features of a typical client's home to the interdisciplinary research team. Once the working version of the virtual simulation training system was created, assessment of its usefulness, usability, and desirability was ongoing to continually develop and modify the system.
Quantitatively, the researchers used the Modified Home Healthcare Worker Questionnaire (MHHWQ) and the usefulness, usability, and desirability (UUD) survey. Qualitative data collection consisted of structured focus groups and individual interviews. The participants described 353 hazard management dilemmas and explained multiple types of “making do” solutions for the hazards, most of which were classified as “less-than-optimal.”
The simulation game facilitated active learning and critical thinking processes crucial for these professionals because they are typically highly autonomous professionals who work independently in unpredictable environments where they must problem solve to create solutions to unforeseen or complex events that affect their health and safety as well as the health and safety of their clients.
To prepare professionals using health and safety trainings, the training must focus on realistic scenarios, flexible solutions, and independent problem-solving activities. The virtual simulation training system includes immersion and engagement through a process of identification, response, problem-solving, and feedback. The professionals had to assess the environment for hazards in several rooms. Then they received feedback about correct identification and right and wrong answers, problem-solving about potential strategies, and assessment of progress in both a training and an evaluation environment; the feedback facilitated deliberate practice, which is a powerful component of skill acquisition.
The researchers concluded that participatory methods are a useful and effective way to design a virtual simulation training system that is interactive, engaging, and informative. Since this project is ongoing, their long-term goal is to improve the health and safety of home healthcare professionals who work in clients' homes.
The full article appears in: Darragh, A., Lavender, S., Polivka, B., Sommerich, C., Wills, C., Hittle, B., Chen, R., & Stredney, D. (2016). Gaming simulation as health and safety training for home health care workers. Clinical Simulation in Nursing, 12(8), 328-335. https://doi.org/10.1016/j.ecns.2016.03.006
|
Virtual Worlds in Education ⬆ ⬇
A 3D virtual world often mimics a real-world environment, although it may also include supernatural abilities, such as flying unaided (Mastrian et al., 2011). Users of virtual worlds are often quick to stress that these creations are not games, although this confusion is easy to understand because virtual worlds share many of the same interface characteristics as 3D action and role-playing games.
The best use of virtual worlds for educational purposes may occur when there is a need for an immersive experience coupled with a need for social interaction. For example, in the virtual world of Second Life, one university has developed a virtual hacienda for students learning Spanish (Clark, 2009). Students interact with the environment and the objects in the hacienda while speaking to one another in Spanish, thereby participating in authentic learning activities. Some of the Second Life scenarios used by a college of nursing include a real human resources representative whom the student must call; the pair must discuss the situation, and the student then determines a solution based on the representative's input. This activity immerses the students in their role and fully engages them in the learning episode. Cohen et al. (2012) tested the use of a virtual world as a training site for emergency preparedness and coordination for first responders in major incidents (e.g., a terrorist attack) and concluded that
[m]ajor incident exercises are complex in nature and expensive and they thereby require novel methodologies to aid training and preparation. This study has established the feasibility of developing low-cost, immersive, accessible virtual environments for major incident preparation using a systematic approach. Both the environment and scenarios were deemed realistic and acceptable for training and testing of existing plans by clinicians. (pp. 83-84)
Virtual worlds need not be 3D. Predecessors to the 3D environment include the multiuser dungeon, object-oriented multiuser dungeon, and multiuser shared hallucination. All of these environments are text based, so the user receives environmental information as passages of text, manipulates objects, and talks to others by typing text commands. Multiuser dungeons, object-oriented multiuser dungeons, and multiuser shared hallucinations are still in use today.
Choosing Among Simulations, Serious Games, and Virtual Worlds ⬆ ⬇
Simulations; educational, or serious, games; and virtual worlds overlap a great deal. Games may be placed in virtual worlds, and simulations may have gamelike elements. Yet these three tools also have distinctive characteristics. By examining several of these key characteristics (i.e., goal orientation, competition, fun factor, exploratory learning, and social interaction), choosing the correct tool for teaching purposes becomes easier.
Games are goal oriented and may be competitive in nature. They should be fun and perhaps a bit fantastical and lighthearted. A particular game may or may not include exploratory learning and social interaction. Although simulations are also goal oriented, the competition is generally subdued. Simulations are typically more realistic and not necessarily fun to use. A particular simulation may or may not include exploratory learning and social interaction. Virtual worlds do not intrinsically have goals or competition; it is up to the player to construct them and add them to the world. Virtual worlds may include fantastical elements. Virtual worlds generally lend themselves to exploratory learning and social interaction. When educators develop virtual worlds for education, they can control the scenarios or activities that the learners experience. Virtual worlds used for simulation also include a debriefing process for their learners, which solidifies the learning.
The Future of Simulations, Serious Games, Virtual Worlds, and the Realities in Nursing Education ⬆ ⬇
The use of simulations, games, and virtual worlds in Western society continues to increase. The combination of best practices supported by sound research, the ever-growing power of technology, and learners who grew up using these environments will lead to greater use of these tools for learning (New Media Consortium, 2007).
In addition, games are becoming less expensive to produce and consume. Game development engines, which were long the exclusive domain of major game development companies, are now available at a cost that many users and organizations can afford. Some games come with built-in development tools, which are the game producers' attempt to use free labor to extend their products (Dyer-Witheford & de Peuter, 2009). The growth of indie (i.e., independent) game companies is leading to a plethora of cheap yet high-quality games. The same holds true for virtual worlds. New virtual worlds spring up all the time. Many offer free (sometimes with limited functionality) accounts, and educators are exploring these spaces with increasing regularity for building fantastic learning environments.
Companies are tapping mobile devices as another avenue to push out their games. These devices are already used for a variety of communication and social functions, so why not expand that platform with casual games that rely on social interactions? Expect to see much more happening in this space in the near future.
Another related area of growth is in augmented-reality games (ARGs). Augmented reality occurs when one uses a device, such as a smartphone, to overlay additional information on the real world (Klopfer & Squire, 2008). For example, one might use the camera in the phone to view the stars at night and see on the phone's screen both the stars and the constellation labels and linking lines between the stars in a constellation. ARGs exploit this concept in gamelike ways, bringing people together physically and virtually to solve a series of challenges. In education, ARGs may be used to provide a fun way to collect and analyze data, collaborate with other students, and access information resources and a new way to look at the world.
Serious games may also have a place in helping practicing nurses maintain or hone skills. Baker (2009) suggested that gaming has a place in continuing education. The science of nursing practice encourages nurses to ask questions, promote dialogue, share lessons learned willingly and openly, and make the outcomes of their patients constructive and positive. Rigorous, high-quality evaluation and research into the teaching and learning techniques offered by serious games can offer insight into future changes not currently conceived of. For example, if a serious game could effectively assist nurses in maintaining the skill set required to care for a patient who is experiencing hypothermia, would that be worth the investment? If a serious game could reduce medication errors in the operating room by 50% to 75% compared to what has been demonstrated in the past, would that have value? If it were found that after implementation of a serious game, a facility experienced zero errors in right-site, right-procedure, and right-patient events during a 10-year period, would this be of value (Baker, 2009, p. 173)?
Serious games can be used to educate health professionals or use their collective knowledge. Foldit (2018) was designed to solve puzzles for science. Foldit had a crowdsourcing computer game that challenged its players to create a protein that could be used as a vaccine for malaria.
The best uses of all these technologies and approaches related to nursing education remain a bit murky (Bauman, 2016, p. 110). Fortunately, the findings of a great deal of research that is currently underway will guide future educators toward the most effective uses of educational games, simulations, and virtual worlds. In an ideal world, educators would have a plethora of available, well-designed, and educator-certified games from which to choose that mesh with the educational objectives of their classes, courses, and curricula.
The two realities of AR and VR are revamping nursing education. They can enhance critical thinking, clinical judgment, and competency and skill attainment. These realities are typically available to the student 24/7 for exploration and practice. As disruptive innovations, they are transforming our educational paradigms and providing interactive, experiential learning. In the future, what is now innovative will be mainstream. Please refer to Chapter 25, Our Expanding Realities and the Metaverse, for more about reality and the realities.
| A Student in the Not Too Distant Future |
|---|
| Dee McGonigle
Nell walks up the steps of the Diamond building on Treemaunt campus. It's a nice day, and she quickly uses her cybervision contacts, or “Cyves,” to check the weather. Appearing before her in midair is a map of the local area, with weather data on her visual periphery. Even though all of the map looks clear, she flicks her eyes toward the data, causing them to move toward her center of vision. Sure enough, there is a 20% chance of rain by 4:00 p.m. Bummer. Nell dismisses her private heads-up display with another flick of her eyes and proceeds into the building. “Oh well,” she muses, “at least I'll be home well before then.”
Nell steps into the classroom for the first time. She's early; only a few other students have preceded her. Sitting down, she again calls up her Cyves and checks her social networks. One friend is at the beach and live broadcasting a view of the tide coming in. Another is at work, lamenting the slow, archaic T9 connection he has to the internet.
More students file in. Nell fires a quick note to her working friend. “Archaic! You should see this classroom! Probably the same chairs my grandmother sat in!”
“Hey!” her friend replies. “I read all about the Diamond building. It may look old, but it's outfitted with the latest stuff. Wait till you get one class in-you'll see!”
Nell takes a moment to review the results of a smart scan she started last night on the upcoming gardening season; correlated for her are a set of recommendations for her gardening efforts this year. It looks like it will be a dry season, so the tomato variety she grew 4 years ago will probably do well, although the report notes that she rated them only a 3 out of 5 on her personal taste scale. The smart scan also lists a number of new tomato varieties she might want to use, inferred from her personal taste scale, which she's added to over the years.
Just then, an older woman enters the room. She is dressed casually but has an air of authority about her. Must be the prof, thinks Nell. A quick scan with her Cyves confirms it. Around the woman springs virtual data, visible only to Nell:
|
- Name: Dr. Janice Stephenson
- Occupation: Professor of Sociology, Treemaunt University
- Hobbies: Golfing and reading
The rest of the data are scrambled. Only people whom Dr. Stephenson has given rights to can view them. “Probably pictures of her cats,” Nell quietly snorts. While Nell is sizing up her professor, the professor is doing the same with the entire class. The professor gives Nell a quick look and a brief smile, leaving Nell a bit disconcerted. What did she read? What DIDN'T she read when she scanned me? Oh boy. “Welcome, class!” begins Dr. Stephenson. As she speaks, a large video screen behind her springs to life, and an avatar of her uses sign language to also greet the class. The text of her voice is also visible above the avatar. Nell realizes that everything is being recorded for everyone to view whenever they want. She always prefers the summary personalized to her learning styles that will be available to her. “This class is an introduction to Treemaunt U and its intelligent enhancements, but it's really more about how to make the most of your experiences here. Many of you probably think this classroom is old fashioned, and until recently, you'd have been correct. But take a closer look. Embedded in each chair is a full connection to the internet. Just push the green button on the side. Go ahead; it's OK,” she prompts. Nell pushes her button and sees her classmates doing the same. Sure enough, a virtual monitor, or air screen, and keyboard appear in the air before her. The chair must have read her public information because it is displaying it just as she views it from her own computer. “Now,” Dr. Stephenson continues, “most of you have Cyves, so you probably don't need this internet access. But it's here for those who do not. You might also notice that the chairs are highly mobile, automatically adjust to your contours, and can be configured in several ways. So breaking up into groups is easy. We can also pull up screens from the floor to partition the room off if need be. Lighting is controllable via several quadrants, making the room very flexible. Imagine what it was like for your parents in college. Can you believe some classrooms had no technology, the chairs were fixed to the floors, and people were actually uncomfortable as they learned? Amazing! Even the classrooms that had technology were limited. Usually, only the professor had access to the video projectors and the internet. In fact, some professors liked it that way. They actually discouraged students from bringing technology to class. I can't imagine how anyone could really learn without the constant access to information we now have. “But I digress. Sure, we all know that learning happens many ways. Hopefully, you'll even find me useful as part of your learning experience. You also have access to sources of information that continue to astound me. Most importantly, you have access to each other. Remember that. “Now, if you look to your right with your Cyves, you will see our virtual eduspace. If you do not have Cyves, use the air screen that popped up when you accessed the internet. The screen will allow you to scan the room like Cyves. You can choose to enter in either two- or three-dimensional mode. Let me know if you cannot see our virtual eduspace. “Everyone seems good to go. Please enter the virtual eduspace, and find your personalized information packet for review. Your parents probably knew this as virtual reality, but we have gone light-years beyond that. If you have not experienced our virtual settings as of yet, please take some time after class to explore. Remember, you will each have a personal preceptor, an artificially intelligent agent, assigned to you. You will meet your preceptor in our virtual eduspace, which will appear as an intelligent avatar, or intellivar, that you can name and customize. You will also decide which channel it will reside on for you. Your preceptor will be with you throughout the program. It will learn how you learn so that it can help you based on your preferences. There are always hidden gems to uncover and new spaces to discover in the virtual territory for this class.” A man three seats to Nell's right raises his hand. “Yes, uh, Joe?” responds Dr. Stephenson. “Meaning no disrespect, Professor, but why do we need classrooms at all? We could all just meet virtually, couldn't we?” “An excellent question, Joe. You're right; we could just meet virtually. We could use Cyves, air screens, or other devices. Yet despite all the wonderful technology we possess, people are still social creatures. We need to be with others, not all the time, but enough so that classrooms are still needed. For this class, we'll meet once a week here. The other two classes will be held in our virtual eduspace. Remember, you can always ask your intellivar to attend a class for you if you are unable to attend. “Other questions? Ah, I see Mary has posed a question on the back channel for the class. For those of you who are new to all this, we use the technology to create another channel of information, a back channel, as the class proceeds. It's a great way to strike while the fire is hot. Your questions and comments are immediately available and addressed. In this case, our back channel is simply text on a web page we can easily display. Let's call it up now.” Dr. Stephenson proceeds to display the back channel page on the video screen. It reads as follows: Mary: I know this is supposed to be an introduction to life as a student, but I'm a transfer student. Do I really need all of this? Dr. Stephenson smiles. “Thirty years ago, you would have been forced to sit through classes where I, the fount of all knowledge and goodness, would have imparted redundant knowledge into your head. Today, we have ways to avoid that. Remember the battery of tests and quizzes you took as part of your entrance process? They're not just busywork. We've used them to put information about you into our learning management system, Aether. The learning management system will work with your intellivar and prescribe things specifically for you here at Treemaunt U, things you might be interested in and things you definitely need. And for things you already know, you'll be given the chance to opt out of them. You will also receive instruction in the forms you like but not all the time. For example, if you like games and there is a game ‘in the open,' meaning it has an Innovative Commons License attached to it so that Treemaunt U can use it legally, and it covers the content you need, guess what? You'll be playing a game! So I believe for you, Mary, there will be some specialized assignments you'll receive-subject to my approval, of course. Maybe I'll even ask you to contribute your information and insights for future classes. Yes, this class and its information are more than just me. They are you. And you, and you, and you. You are all part of the process, so be prepared to be active participants in your learning, not just passive recipients. “OK, we could probably get through today's class just with me answering your questions, but why don't I go ahead with my outline and whatever I don't cover we can talk about afterward. Oh, and please turn your friend alerts off or on color alert. I know some of you have to take calls and such, but please respect me and your classmates.” The preceding story was a tiny slice of the many possibilities the future holds. It does not begin to touch on the opportunities that nanotechnology, cheap fusion power, or what embedded communication devices might bring to education. Instead, it concentrated on the more tangible possibilities that are logical extensions of what we can do today. The following key elements are alluded to in the story: - Back channels
- Cyves
- Next-generation morphing classrooms
- Advanced web technologies, social networking, user-created content, and collective intelligence
- Intellivars
- Cloud computing
- Semantic-aware applications
- Smart objects
- Open source technologies
- Learning management systems (LMSs)
- Personal learning environments (PLEs)
- Personalized learning
- Adaptive learning
- Specialized educational modules delivered just in time
- Mobile devices
- Virtual eduspaces; virtual worlds; simulations; and educational, or serious, games
|
| Cyves Definition |
|---|
| Cyves stands for computerized yagi visual earshot sensations. They are computer processors embedded in contact lenses equipped with a visual display as well as auditory channels for communicating. A yagi is a sharply directional antenna. |
Realities ⬆ ⬇
The realities have been described as disruptive innovations (see the Disruptive Innovations box). Using virtual realities in education requires immersion. The expectation of immersive learning is that learners will become absorbed, engrossed, and engaged in the learning activity to the point that they suspend their own reality and truly experience the virtual scenarios and simulations as if they were real; they feel that they are actually participating in a physical setting instead of the virtual, synthetic, artificially generated environment. Augmented reality (AR) and virtual reality (VR) are technological examples of immersive environments used in learning episodes to enhance the learning experience in a safe setting.
Augmented Reality
Augmented reality (AR) is an interactive experience within a real-world environment that enhances real-world objects using virtually simulated, or computer-generated, perceptual information. Integrating AR into educational venues provides stimulation, or input, for multiple senses, including olfactory, visual, auditory, haptic, and somatosensory (e.g., pressure, pain, or warmth). It comprises apps; wearable technologies, such as glasses; and software that not only interacts with users but also enhances their senses with data, information, audio, and images.
| Disruptive Innovations |
|---|
| Disruptive innovations are new developments that radically change, or disrupt, the way structures or industries function. They are the introductions of products or services into well-known or established industries that outperform all other products or services (i.e., are more efficient and lower priced), thereby obtaining competitive advantages, which capture the market share and alter and transform those industries.
Thinking about the internet, how did it disrupt education? Examples of disruptive innovations that are game changers follow. Reflect on each of them, the disruption they have caused as they evolved and how their disruption affects nursing education.
|
- Surgeon using VR to practice a surgery using the patient's own anatomy so that in the actual surgery, the risk of the surgeon being met with an unanticipated event is minimized. Will this preparation be the norm for all surgeries going forward? If so, how do we educate current practitioners and students who will be the future healthcare professionals in the workforce?
- Artificial intelligence (AI)
- Internet of Things (IoT) and Artificial Intelligence of Things (AIoT)
- Blockchain technology
- Robotics
What other disruptive innovations can you think of, and why were or are they disruptive, or game changers? |
AR does not require specialized equipment; the digital information is overlaid on an image of something being viewed through a smart device's camera. AR has been integrated into nursing curriculums to help nursing students achieve and improve clinical skill proficiency. AR improves the abstract, or conceptual, comprehension of phenomena. Faculty members can bring abstract concepts to life with AR expeditions in which they and the students actively explore. Learners can view and manipulate digital animations, such as a beating heart or human brain, by bringing them into their real background. This helps nursing students understand the relationships of diseases and normal pathophysiology. Nursing students can also better understand the effect of procedures in relation to the anatomy and physiology of their patients. AR is a learning experience that enhances critical thinking skills and clinical judgment.
Virtual Reality
Virtual reality (VR) is infiltrating health care to improve plans of care and patients' outcomes. Heady (2019) described the use of VR at the University of California at Los Angeles to explore the patient's own anatomy prior to surgery. VR “models to prepare for kidney tumor surgeries resulted in substantial improvements, including shorter operating times, less blood loss during surgery and a shorter stay in the hospital afterward” (para. 1). VR is also being used to distract patients during painful and/or lengthy procedures, such as helping patients stay relaxed and comfortable while receiving chemotherapy (Pratt, 2017), and for pain management. Brody (2019) said that for pain management, it is more than a distraction: “It's more like a brain hack that occupies the brain so fully that it has no room to process pain sensations at the same time” (para. 1). “Through the hospital's [Stanford Medicine Children's Health] CHARIOT program [www.stanfordchildrens.org/en/innovation/chariot], Packard Children's is one of the only hospitals in the world to have VR available on every unit to help engage and distract patients undergoing a range of hospital procedures” (Stanford Medicine Children's Health, n.d., para. 2). VR integrations such as these demand that nurse educators prepare nurses to function in environments that expand into VR so that they can actively participate in the evolution of the technologies being used to enhance patient care.
See Research Brief 3, which discusses VR airway research. Dr. McGonigle worked with the students and faculty as they experienced the VR airway lab during this research project; she felt their excitement and how they reacted to the immersive VR environment. Based on this type of research, innovative nurse educators and experts in nursing education and informatics are designing VR scenarios and simulations for nursing students. The VR learning episodes exist in a controlled virtual environment that immerses nursing students in the educational experience. They are able to practice and learn by doing in VR and are being familiarized to this technology.
| Toward a Virtual Future of Medical Simulation |
|---|
| Medical simulation is a vitally important learning modality and has been proven to reduce errors, improve patient outcomes, and save lives. However, access remains relatively expensive and dependent on the physical hardware space of simulation centers and high-fidelity mannequins. Virtual technologies offer the opportunity to massively expand access to medical simulation to anyone, anywhere, anytime.
Following the trend of so many industries touched by virtualization, medical simulation is beginning to realize a similar trajectory. The physical infrastructure required to support industries such as film, newspapers, music, and magazines is an example of this transcendence into digital counterparts. In each case, this transition substantially lowered costs and increased access while introducing explosive new growth opportunities that were never before possible. The same will be true of medical simulation.
Virtual counterparts to the physical “stuff” of simulation are already growing rapidly as numerous studies validate their efficacy. Perhaps most importantly, those who never before had access will soon enjoy expansive libraries of digital environments, equipment, patients, and scenarios to advance their hands-on and critical thinking skills.
Virtual simulation also introduces powerful network effects by building bridges between experts and participants joining from rural or remote locations. The simulation center of the future is no longer an isolated physical location but rather an interconnected node with real-time access to a perpetually evolving library of expertise and validated best practices.
Virtualization also enables simulation to take lateral steps and expand beyond an isolated scenario narrative into a broader chronology of events that are more akin to the realities of clinical experience. It can more easily bridge between professions, thus enabling cross-disciplinary training on a level that has never before been possible.
Looking ahead to the future of virtual simulation, we may begin to completely rethink and expand its role far beyond what is familiar today. Moving beyond the mere simulation, we might envision fictitious patients and scenarios transitioning into a mirror world of real-time patient interactions that span the entire spectrum of health care.
Patients in the future might opt in to maintain a real-time, digital counterpart of themselves and thus enable procedures to be rehearsed virtually. Imagine an emergency room team rehearsing lifesaving procedures on a patient's virtual replica, trying different approaches and realizing potential complications long before the ambulance arrives.
|
 A three-dimensional simulated scenario portrays three healthcare professionals watching over a patient lying on a bed in a room. An E C G monitor is present beside the patient. A three-dimensional simulated healthcare scenario depicts two healthcare professionals overseeing a patient lying in a semi-Fowler's position on a bed in a room. Screens on the walls display E C G, heart and other medical data. A three-dimensional simulated healthcare scenario depicts two healthcare professionals having a discussion in a hospital room, standing in front of a ventilator and an E C G monitor. 
A three-dimensional simulated healthcare scenario depicts a healthcare team attending to a child patient lying on a bed in an operating theater. A three-dimensional simulated healthcare scenario depicts a healthcare team having a discussion in an empty operating theater, with surgical tools and equipment neatly laid out on a table. Actual image from Acadicus. Inclusion in this text was permitted by Jon Brouchoud, CEO, Arch Virtual, Developers of Acadicus |
| Research Brief 3 Teaching Airway Insertion Skills to Nursing Faculty and Students Using VR: A Pilot Study |
|---|
| Purpose of Investigation |
|---|
| To examine whether an educational intervention with a pilot contemporary immersive virtual reality simulation (CIVRS) builds knowledge and is feasible to implement among nursing students and faculty. |
| Intervention |
|---|
| VR airway lab intervention with six adjunct narrated lessons: |
- Bag valve mask
- Oropharyngeal airway
- Nasopharyngeal airway
- King laryngeal airway tube
- Laryngeal mask airway
- Endotracheal tube
|
| Survey Sampling |
|---|
| N = 31 (10 faculty members and 21 students) |
| Theoretical Framework |
|---|
- Bauman's Layered-Learning model
- Situated and multimodal approach
- Knowledge building occurs by leveraging contemporary educational technologies
- Scaffolding knowledge transfer for learners
- Faculty roles shift to facilitate users' discovery of knowledge
- Technology enhances opportunities for mastery learning, moving learners from didactic preparation to and through the simulation to the practice pathway
|
| Methodology |
|---|
- Survey sampling
- Quasi-experimental
- One-group pre- and posttest design
|
| Approach |
|---|
- Enact the VR intervention
- Virtual Presence Questionnaire
- Virtual Reality Sickness Questionnaire
- Knowledge test
|
| Results |
|---|
| Faculty and students rated the VR airway lab as having a high level of virtual presence and reported no cybersickness and significant improvement of knowledge of airway management (p 0.0001). |
| Conclusions |
|---|
- The VR airway lab was an efficacious means of teaching difficult airway management skills to nursing students.
- A VR airway intervention was presented to teach difficult airway management using six different airway adjuncts.
- Students and faculty widely accepted the intervention.
- The researchers recommended that further research be conducted to evaluate this immersive, educational delivery medium.
|
Summary ⬆ ⬇
Simulated experiences in nursing education contain the PEDA elements, which provide important opportunities for students to hone critical thinking and clinical judgment skills in a safe and supportive environment. Simulation scenarios may also provide a better variety of clinical and practicum experiences than those available in a real setting, and they also provide nursing faculty the opportunity to track student progress and development against specific learning objectives. Nurse educators can share simulation scenarios and experiences and thus contribute to the body of nursing education knowledge to improve education practice. Simulations; games; virtual worlds; and the realities, AR and VR, have a great deal of potential as educational tools for augmenting, supplementing, or even replacing traditional methods of teaching as well as clinical experiences. As educators become more skilled in the use of these tools; designers share their creative works with others; and nurse informaticists lead, collaborate, and support these efforts, we can expect to see these tools blended, honed, integrated, and leveraged more frequently in the coming decade.
| Thought-Provoking Questions |
|---|
- Consider your experience and learning regarding EHRs. If you were to design a learning program centered on the use of EHRs, what would it look like? Consider this from the viewpoint of an educator, a student, a clinician, and a healthcare administrator.
- Think about the clinical courses you have taken as a student. Which opportunities and challenges exist regarding the use of an EHR as a major learning tool in conjunction with, or perhaps even replacing, the required textbook?
- If you were to design a simulation scenario incorporating the use of an EHR, which informatics competencies would you focus on and why?
- Games are supposed to be fun and voluntary. How can educators force a game on a student and expect it to remain fun and engaging?
- It can take several hours of gameplay to learn the mechanics of some games and even longer for the more complex games. If subject matter learning can occur only after this initial game mechanics learning occurs, how can educators justify the amount of time a learner must spend within the game just to get to the point where learning begins?
- If you were choosing between a latex-based and a virtual simulation, what would you list as each of their advantages and disadvantages? Would PEDA elements be present for both?
- How do educators acquire the training needed not just to get by in these new environments but to flourish, thrive, and mold the environments for their purposes?
- What realities have you experienced? Describe your experience in detail. If you have not experienced any realities, imagine how AR and VR could affect your education and/or clinical practice setting.
|
References ⬆
- Aebersold M., & Tschannen D. (2013). Simulation in nursing practice: The impact on patient care. Online Journal of Issues in Nursing, 18(2). https://doi.org/10.3912/OJIN.Vol18No02Man06
- Aldrich C. (2010, August). Virtual worlds, simulations and games for online educators. Magna online seminar presented at Penn State University, University Park, PA.
- Alessi S. M. (1988). Fidelity in the design of instructional simulations. Journal of Computer-Based Instruction, 15(2), 40-47.
- American Academy of Nursing. (2003). Proceedings of the American Academy of Nursing conference on using innovative technology to decrease nursing demand and enhance patient care delivery.Nursing Outlook, 51(3), S1-S41.
- American Association of Colleges of Nursing. (1999). A vision of baccalaureate and graduate nursing education: The next decade [position statement].Journal of Professional Nursing, 15(1), 59-65. https://doi.org/10.1016/S8755-7223(99)80027-1
- American Nurses Association. (2014). Nursing informatics: Scope and standards of practice (2nd ed.). Nursebooks.org
- Baker J. (2009). Serious games and perioperative nursing. AORN Journal, 90(2), 173-175. https://doi.org/10.1016/j.aorn.2009.07.002
- Bauman E. (2016). Games, virtual environments, mobile applications and a futurist's crystal ball. Clinical Simulation in Nursing, 12, 109-114. https://doi.org/10.1016/j.ecns.2016.02.002
- Bligh J., & Bleakley A. (2006). Distributing menus to hungry learners: Can learning by simulation become simulation of learning? Medical Teacher, 28(7), 606-613. https://doi.org/10.1080/01421590601042335
- Brody J. (2019, April 29). Virtual reality as therapy for pain. New York Times. www.nytimes.com/2019/04/29/well/live/virtual-reality-as-therapy-for-pain.html
- Carty R., & Ong I. (2006). The nursing curriculum in the information age. In V. K.Saba & K. A.McCormick (Eds.), Essentials of nursing informatics (4th ed., pp. 517-531). McGraw-Hill.
- Chen Y. (2012). Evaluation of MTA learning achievement based on rule-space model and relevance feedback with e-Learning. Journal of Computers, 23(1).
- Choi M., Park J., & Lee H. (2016). Assessment of the need to integrate academic electronic medical records into the undergraduate clinical practicum. CIN: Computers, Informatics, Nursing, 34(6), 259-265. https://doi.org/10.1097/CIN.0000000000000244
- Clark G. (2009). These horses can fly! and other lessons from Second Life: The view from the virtual hacienda. In R.Oxford & J.Oxford (Eds.), Second language teaching and learning in the Net Generation (pp. 153-172). National Foreign Language Resource Center.
- Cohen D., Sevdalis N., Taylor D., Kerr K., Heys M., Willett K., Batrick N., & Darzi A. (2012). Emergency preparedness in the 21st century: Training and preparation modules in virtual environments. Resuscitation, 84(1), 78-84. https://doi.org/10.1016/j.resuscitation.2012.05.014
- Connors H. R., Weaver C., Warren J., & Miller K. L. (2002). An academic-business partnership for advancing clinical informatics. Nursing Education Perspectives, 23(5), 228-233.
- Csikszentmihalyi M. (1990). Flow: The psychology of optimal experience. HarperCollins.
- Darragh A., Lavender S., Polivka B., Sommerich C., Wills C., Hittle B., Chen R., & Stredney D. (2016). Gaming simulation as health and safety training for home health care workers. Clinical Simulation in Nursing, 12(8), 328-335. https://doi.org/10.1016/j.ecns.2016.03.006
- Dyer-Witheford N., & de Peuter G. (2009). Games of empire: Global capitalism and video games. University of Minnesota Press.
- Fetter M. (2009). Graduating nurses' self-evaluation of information technology competencies. Journal of Nursing Education, 48(2), 86-90. https://doi.org/10.3928/01484834-20090201-05
- Fisher R. (2016). Designing the simulation learning environment: An active engagement model. Journal of Nursing Education and Practice, 6(3), 6-14. https://doi.org/10.5430/jnep.v6n3p6
- Foldit. (2018, April 10). 1507: Malaria vaccine design. https://fold.it/portal/node/2005024
- Gaba D. (2004). The future vision of simulation in health care. BMJ Quality and Safety, 13, i2-i10. http://dx.doi.org/10.1136/qshc.2004.009878
- Gaba D., & DeAnda A. A. (1998). A comprehensive anesthesia simulation environment: Recreating the operating room for research and training. Anesthesiology, 69(3), 387-394. https://doi.org/10.1097/00000542-198809000-00017
- Gassert C. A. (1998). The challenge of meeting patients' needs with a national nursing informatics agenda. Journal of the American Medical Informatics Association, 5(3), 263-268. https://doi.org/10.1136/jamia.1998.0050263
- Gredler M. E. (1996). Educational games and simulations: A technology in search of a (research) paradigm. In D. H.Jonassen (Ed.), Handbook of research for educational communications and technology (pp. 521-540). Lawrence Erlbaum.
- Harris J., Shoemaker K., Johnson K., Tompkins-Dobbs K., & Domian E. (2016). Qualitative descriptive study of family nurse practitioner student experiences using high-fidelity simulation. The Kansas Nurse, 91(2), 12-15.
- Harris S. (2020). Silicone skin trays: An innovative simulation approach to nurse practitioner skills training. Clinical Simulation in Nursing, X, 1-4. https://doi.org/10.1016/j.ecns.2020.05.002
- Hayden J. K., Smiley R. A., Alexander M., Kardong-Edgren S., & Jeffries P. R. (2014). The NCSBN National Simulation Study: A longitudinal, randomized, controlled study replacing clinical hours with simulation in prelicensure nursing education. Journal of Nursing Regulation, 5(Suppl. 2), S3-S40. https://doi.org/10.1016/S2155-8256(15)30062-4
- Heady D. (2019, September 18). 3D virtual reality models help yield better surgical outcomes. UCLA Newsroom. https://newsroom.ucla.edu/releases/3d-virtual-reality-models-improve-surgical-outcomes
- Healthcare Information and Management Systems Society. (n.d.). Technology informatics guiding education reform (TIGER). www.himss.org/tiger-initiative-technology-and-health-informatics-education
- Hertel J. P., & Millis B. J. (2002). Using simulations to promote learning in higher education: An introduction. Stylus.
- Hunter K., McGonigle D., & Hebda T. (2013). TIGER-based measurement of nursing informatics competencies: The development and implementation of an online tool for self-assessment. Journal of Nursing Education and Practice, 3(12), 70-80. https://doi.org/10.5430/jnep.v3n12p70
- Institute of Medicine. (2000). To err is human: Building a safer system. National Academies Press.
- Jonassen D. H. (1999). Designing constructivist learning environments. In C. M.Reigeluth (Ed.), Instructional design theories and models: A new paradigm of instructional theory (Vol. 2, pp. 215-239). Lawrence Erlbaum.
- Kelley D. (1988). The art of reasoning. W. W.Norton .
- Kennedy D., Pallikkathayil L., & Warren J. J. (2009). Using a modified electronic health record to develop nursing process skills. Journal of Nursing Education, 48(2), 96-100. https://doi.org/10.3928/01484834-20090201-07
- Klopfer E., & Squire K. (2008). Environmental detectives: The development of an augmented reality platform for environmental simulations. Education Technology Research and Development, 56, 203-228. https://doi.org/10.1007/s11423-007-9037-6
- Koster R. (2004). A theory of fun for game design. Paraglyph Press.
- Mahon P. Y., Nickitas D. M., & Nokes K. M. (2010). Faculty perceptions of student documentation skills during the transition from paper-based to electronic health records systems. Journal of Nursing Education, 49(11), 615-621. https://doi.org/10.3928/01484834-20100524-06.
- Mastrian K. G., McGonigle D., Mahan W. L., & Bixler B. (2011). Integrating technology in nursing education: Tools for the knowledge era. Jones & Bartlett Learning.
- McGonigle D., Hunter K., Hebda T., & Hill T. (2013). Self-assessment of level 3 and level 4 NI competencies tool development. https://sigma.nursingrepository.org/bitstream/handle/10755/623941/ToolAssessment.pdf?sequence=1&isAllowed=y
- Mungai D., Jones D., & Wong L. (2002, August). Games to teach by. Paper presented at the 18th Annual Conference on Distance Teaching and Learning, Madison, WI.
- Murray S. (2019, March 3). Moocs struggle to lift rock-bottom completion rates. Financial Times. www.ft.com/content/60e90be2-1a77-11e9-b191-175523b59d1d
- National League for Nursing. (2015, January). A vision for the changing faculty role: Preparing students for the technological world of healthcare. www.nln.org/docs/default-source/uploadedfiles/about/nln-vision-series-position-statements/a-vision-for-the-changing-faculty-role-preparing-students-for-the-technological-world-of-health-care.pdf
- Nemerow L. G. (1996). Do classroom games improve motivation and learning? Teaching and Change, 3(4), 356-366.
- New Media Consortium. (2007). Massively multiplayer educational gaming.The Horizon Report, 25-27. https://thecurrent.educatorinnovator.org/sites/default/files/files/119/2007%20Horizon%20Report.pdf
- Pew Health Professions Commission. (1998). Recreating health professional practice for a new century: The fourth report of the Pew Health Professions Commission. https://healthforce.ucsf.edu/sites/healthforce.ucsf.edu/files/publication-pdf/3.1%20%28Report%29%201998-12_Recreating_Health_Professional_Practice_for_a_New_Century_The_Fourth_Report_of_the_Pew_Health_Professions_Commission.pdf
- Podolefsky N. S., Moore E. B., & Perkins K. K. (2013). Implicit scaffolding in interactive simulations: Design strategies to support multiple educational goals. arXiv. https://arxiv.org/pdf/1306.6544.pdf%3B
- Pratt E. (2017, March 9). VR and chemotherapy for cancer patients. VR Fitness Insider. www.vrfitnessinsider.com/vr-chemotherapy-cancer-patients
- Prensky M. (2001). Digital game-based learning. McGraw-Hill.
- Rajalahti E., Heinonen J., & Saranto K. (2014). Developing nurse educators' computer skills towards proficiency in nursing informatics. Informatics for Health and Social Care, 39(1), 47-66. https://doi.org/10.3109/17538157.2013.834344
- Raths D. (2020, May 22). Vanderbilt Center builds bridge between informatics researchers, applied IT. Healthcare Innovation. www.hcinnovationgroup.com/clinical-it/electronic-health-record-electronic-medical-record-ehr-emr/article/21139450/vanderbilt-clinical-informatics-center-builds-bridge-between-academic-informatics-applied-it
- Robinson-Reilly M., Irwin P., Coutts R., & Slattery N. (2020). Adding telehealth simulation into NP programs. The Nurse Practitioner, 45(3), 44-49. https://doi.org/10.1097/01.NPR.0000653956.29721.1a
- Salen K., & Zimmerman E. (2003). Rules of play: Game design fundamentals. MIT Press.
- Staggers N., Gassert C. A., & Curran C. (2002). A Delphi study to determine informatics competencies for nurses at four levels of practice. Nursing Research, 51(6), 383-390.
- Stanford Medicine Children's Health. (n.d.). Virtual reality and immersive technologies at Stanford Children's Health.www.stanfordchildrens.org/en/innovation/virtual-reality
- Stuart S. (2018, August 8). Here come the virtual humans. PCMag. www.pcmag.com/news/here-come-the-virtual-humans
- Tanner C. (2006). Thinking like a nurse: A research-based model of clinical judgment in nursing. Journal of Nursing Education, 45(6), 204-211. http://dx.doi.org/10.3928/01484834-20060601-04
- Woroch R., Alvarez D., Yingling C., & Handrup C. (2018). Family nurse practitioner/psychiatric mental health nurse practitioner collaboration in drug-seeking telephone triage simulation in an advanced practice registered nurse curriculum. Clinical Simulation in Nursing, 18, 14-19. https://doi.org/10.1016/j.ecns.2018.01.002