Glare and blurred vision, worse on awakening. May progress to severe pain due to ruptured bullae. Symptoms usually develop in the fifth and sixth decades.
Critical
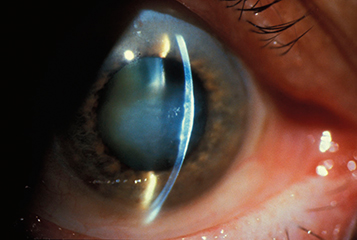
Cornea guttae with stromal ± epithelial edema (see Figure 4.27.1). Bilateral, but may be asymmetric.
Figure 4.27.1: Corneal edema secondary to Fuchs endothelial dystrophy.
|
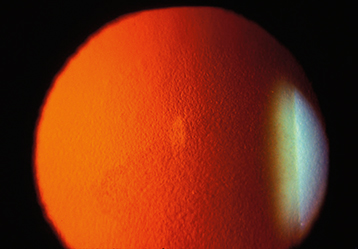
 NOTE NOTECentral cornea guttae without stromal edema is called endothelial dystrophy (see Figure 4.27.2). This condition may progress to Fuchs dystrophy over years. |
Figure 4.27.2: Corneal guttae in endothelial dystrophy.
Other
Fine pigment dusting on the endothelium, central epithelial edema and bullae, folds in Descemet membrane, stromal edema, subepithelial haze, or scarring.
Every 3 to 12 months to check IOP and assess corneal edema. The condition progresses very slowly, and visual acuity typically remains good until stromal edema, epithelial edema, and/or corneal scarring develop.