Slowly progressive visual loss or blurring, usually over months to years, affecting one or both eyes. Glare, especially in bright sun or from oncoming headlights while driving at night, and altered color perception may occur, but not to the same degree as in optic neuropathies. Characteristics of the cataract determine specific symptoms.
(See Figure 13.1.1.)
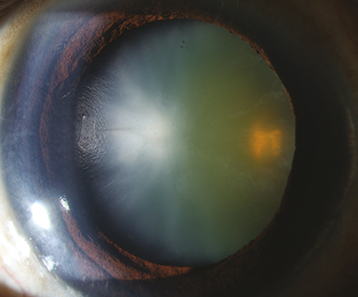
Figure 13.1.1: Cataract with early cortical changes and nuclear sclerosis.
Critical
Opacification or discoloration of the normally clear crystalline lens.
Other
Blurred view of the retina with dimming or disruption of the red reflex on retinoscopy. Myopic shift from nuclear sclerosis may cause increased near vision—so-called “second sight.” Cataract alone does not cause a relative afferent pupillary defect (RAPD).
Determine the etiology, whether the cataract is responsible for the decreased vision, and whether surgical removal would improve vision.
History: Medications (e.g., tamsulosin and other drugs used for urinary retention [alpha-1 antagonists] strongly associated with intraoperative floppy iris syndrome)? Systemic diseases? Trauma? Ocular disease or poor vision before the cataract?
Complete ocular examination, including distance and near vision, pupillary examination, and refraction. When best-corrected acuity is 20/30 or better, glare testing is helpful to demonstrate decreased vision. A dilated slit-lamp examination using both direct and retroillumination techniques is required to view the cataract properly. Fundus examination, concentrating on the macula, is essential in ruling out other causes of decreased vision.
For preoperative planning, note the degree of pupil dilation, density of the cataract, and presence or absence of pseudoexfoliation, phacodonesis (quivering of the lens indicating zonular damage or weakness), or corneal guttae.
B-scan ultrasound (US) if the fundus is not visible to rule out detectable posterior segment disease.
The potential acuity meter (PAM) or laser interferometry can be used to estimate the visual potential when cataract extraction is considered in an eye with posterior segment disease.
|
 NOTE NOTEPAM and laser interferometry often overestimate the eye’s visual potential in the presence of macular holes or macular pigment epithelial detachments. Interferometry also overestimates visual potential in cases of amblyopia. Near vision is often the most accurate manner of evaluating macular function if the cataract is not too dense. Nonetheless, both PAM and laser interferometry are useful clinical tools. |
Keratometry readings and measurement of axial length are required for determining the power of the desired intraocular lens (IOL). Corneal pachymetry or endothelial cell density is occasionally helpful if corneal guttae are present.
Unless there is a secondary complication from the cataract (e.g., glaucoma), a cataract itself does not require urgent action. If a patient requires bilateral cataract extraction, surgery is typically first performed on the more advanced cataract. Patients who decline surgical removal are reexamined annually or sooner if symptoms worsen.
If congenital, see 8.12, Pediatric Cataract.