(See Figure 11.21.1.)
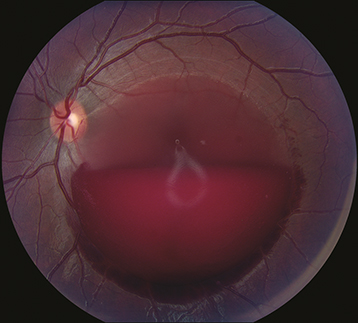
Single or multiple hemorrhages under the ILM in the area of the macula. Can be unilateral or bilateral. Blood may turn yellow after a few days.
Vitreous, intraretinal, subretinal, and subconjunctival hemorrhage can occur.
Decreased vision or asymptomatic. History of Valsalva maneuver (forceful exhalation against a closed glottis), which may occur during heavy lifting, coughing, vomiting, or straining during bowel movement. Sometimes, no history of Valsalva can be elicited.
(See Figure 11.21.1.)
Single or multiple hemorrhages under the ILM in the area of the macula. Can be unilateral or bilateral. Blood may turn yellow after a few days.
Vitreous, intraretinal, subretinal, and subconjunctival hemorrhage can occur.
PVD: Can cause VH acutely as well as peripheral retinal and disc margin hemorrhages. However, sub-ILM hemorrhage is rare. See 11.1, Posterior Vitreous Detachment.
RAM: Hemorrhages in multiple layers of the retina and vitreous. Can also have a circinate ring of hard exudates around a macroaneurysm. See 11.19, Retinal Arterial Macroaneurysm.
Diabetic retinopathy: Microaneurysms, dot-blot hemorrhages, and hard exudates bilaterally. No isolated sub-ILM hemorrhage. Can also cause VH. See 11.12, Diabetic Retinopathy.
CRVO or BRVO: Unilateral, multiple intraretinal hemorrhages, venous dilation, and tortuosity. See 11.8, Central Retinal Vein Occlusion and 11.9, Branch Retinal Vein Occlusion.
Anemia or leukemia: May have multiple, bilateral flame and dot-blot hemorrhages as well as CWSs. Can also present with sub-ILM hemorrhage.
RT: Can be surrounded by hemorrhage obscuring the tear. Tears rarely occur in the macula.
Valsalva causes sudden increase in intraocular venous pressure leading to rupture of superficial capillaries in macula or elsewhere in the retina. May be associated with anticoagulant therapy.
History: History of Valsalva including any recent heavy lifting, straining during bowel movement, coughing, sneezing, vomiting, etc.? The patient may not remember the incident.
Complete ocular examination, including dilated fundus examination with a slit lamp and a handheld lens, and indirect ophthalmoscopy. Look for findings suggestive of a different etiology including microaneurysms, dot-blot hemorrhages, CWSs, RT, PVD.
If dense VH is present, perform a B-scan US to rule out RT or RD.
IVFA may be helpful to rule out other causes including RAM or diabetic retinopathy.
Prognosis is excellent. Most patients are observed, as sub-ILM hemorrhage usually resolves after a few days to weeks. Occasionally laser is used to permit the blood to drain into the vitreous cavity, thereby uncovering the macula. Vitrectomy rarely needed, typically only for nonclearing VH.