(See Figure 11.5.1.)
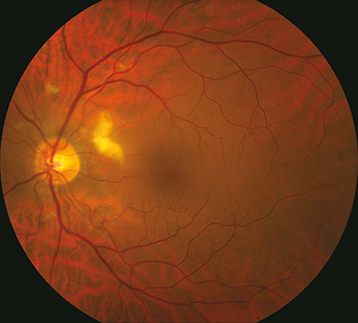
Localized whitening in the superficial retinal NFL with fluffy appearance to margins.
(See Figure 11.5.1.)
Localized whitening in the superficial retinal NFL with fluffy appearance to margins.
Retinal whitening secondary to infectious retinitis, such as that seen in toxoplasmosis, herpes simplex virus, varicella zoster virus, and cytomegalovirus. These entities typically have vitritis and retinal hemorrhages associated with them. See 12.9, Toxoplasmosis and 12.13, Acute Retinal Necrosis.
Myelinated NFL: Develops postnatally. Usually peripapillary but may be in retinal areas remote from the disc (See Figure 11.5.2).
Thought to be an acute obstruction of a precapillary retinal arteriole causing blockage of axoplasmic flow and subsequent buildup of axoplasmic debris in the NFL.
Diabetes mellitus: Most common cause. Often associated with microaneurysms, dot-blot hemorrhages, and hard exudates. See 11.12, Diabetic Retinopathy.
Chronic or acute HTN: May see retinal arteriolar narrowing and flame hemorrhages in chronic HTN. Acute HTN may have hard exudates, optic nerve swelling, exudative RD. See 11.10, Hypertensive Retinopathy.
RVO: Unilateral, multiple hemorrhages, venous dilation, and tortuosity. Multiple CWSs, usually ≥6, seen in ischemic varieties. See 11.8, Central Retinal Vein Occlusion and 11.9, Branch Retinal Vein Occlusion.
Retinal emboli: Often from carotid arteries or heart with resulting ischemia and subsequent CWS distal to arterial occlusion. Patients require carotid Doppler examination and echocardiography. See 10.22, Transient Visual Loss/Amaurosis Fugax.
Collagen vascular disease: Systemic lupus erythematosus (most common), granulomatosis with polyangiitis (formerly Wegener granulomatosis), polyarteritis nodosa, scleroderma, etc.
Giant cell arteritis (GCA): Age ≥55 years. Symptoms include vision loss, scalp tenderness, jaw claudication, proximal muscle aches, etc. See 10.17, Arteritic Ischemic Optic Neuropathy (Giant Cell Arteritis).
HIV retinopathy: Single or multiple CWSs in the posterior pole. See 12.11, HIV Retinopathy.
Other infections: Toxoplasmosis, orbital zygomycosis, Lyme disease, leptospirosis, Rocky Mountain spotted fever, onchocerciasis, subacute bacterial endocarditis, others.
Hypercoagulable state: Polycythemia, multiple myeloma, cryoglobulinemia, Waldenström macroglobulinemia, antiphospholipid syndrome, factor V Leiden, activated protein C resistance, hyperhomocysteinemia, protein C and S deficiency, antithrombin III mutation, prothrombin mutation, etc.
Radiation retinopathy: Follows radiation therapy to the eye or periocular structures when the eye is irradiated inadvertently. May occur any time after radiation, but occurs most commonly within a few years. Maintain a high suspicion even in patients in whom the eye was reportedly shielded. Usually, 3,000 cGy is necessary, but it has been noted to occur with 1,500 cGy. Resembles diabetic retinopathy.
Purtscher and pseudo-Purtscher retinopathy: Multiple CWSs and/or superficial hemorrhages in a peripapillary configuration. Typically bilateral but can be unilateral and asymmetric. See 3.16, Purtscher Retinopathy.
Others: Migraine, hypotension, intravenous drug use, papilledema, papillitis, severe anemia, sickle cell, acute blood loss, etc.
History: Diabetes or HTN? Prior ocular or periocular radiation? GCA symptoms in appropriate age group? Symptoms of collagen vascular disease including joint pain, rashes, etc.? HIV risk factors? Hematologic abnormalities?
Complete ocular examination, including dilated fundus examination with a slit lamp and a handheld lens and indirect ophthalmoscopy. Look for concurrent hemorrhages, vascular occlusion, vasculitis, hard exudates.
Consider erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and platelets if GCA suspected.
Consider blood and urine cultures, chest x-ray, carotid and orbital Doppler examination, chest computed tomography (CT), and echocardiography if emboli are suspected.
Fluorescein angiography is often not helpful for an isolated CWS without concomitant pathology. IVFA can reveal areas of capillary nonperfusion adjacent to CWS location.