AC cell and flare, vitreous cell and haze, vascular sheathing, choroidal, chorioretinal, and choroidal lesions.
Reactive eyelid edema, ciliary injection, KP, iris nodules, peripheral anterior synechiae, cataract, exudative retinal detachment, and papillitis.
Diagnostic Categories
ARN: Most commonly secondary to VZV or HSV infection. Presents as large swaths of confluent retinitis that rapidly progresses and is typically associated with significant vitritis and anterior uveitis. Significant AC reaction may or may not be present. Vitritis is typically not severe. See 12.13, Acute Retinal Necrosis.
Bacterial endogenous endophthalmitis: May have associated severe AC reaction, hypopyon, and/or fibrin. Severe vitritis. May have limited view of posterior segment. See 12.17, Endogenous Bacterial Endophthalmitis.
TB: Produces varied clinical manifestations. The diagnosis is usually made by ancillary laboratory tests and response to antituberculosis therapy. Miliary TB may produce multifocal, small, yellow-white choroidal lesions. Most patients have concomitant anterior granulomatous or nongranulomatous uveitis.
Syphilis: Pleomorphic uveitis. May present as a nonspecific panuveitis with or without more recognizable morphologies such as posterior placoid syphilis and punctate inner retinitis. See 12.10, Syphilis.
Fungal endogenous endophthalmitis: Most commonly caused by Candida or Aspergillus species. Vitritis and AC reactions are typically not as severe as bacterial etiologies. See 12.18, Endogenous Fungal Endophthalmitis.
Toxoplasmosis: Typically a unilateral retinal lesion that may or may not be associated with an adjacent pigmented chorioretinal scar. Associated with a dense vitritis over an area of white retinitis creating the classic “headlight in a fog” appearance. AC reaction is variable. See 12.9, Toxoplasmosis.
Toxocariasis: Almost exclusively unilateral. Three forms: (1) Panuveitis—occurs in children aged 2 to 9 years, often times asymptomatic with dense vitritis, (2) Posterior pole granuloma, occurs in children from age 6 to 14 years, (3) Peripheral retinal granuloma with secondary vitritis and tractional retinal bands, occurs in those aged 6 to 40 years. All three forms can progress to retinal detachment.
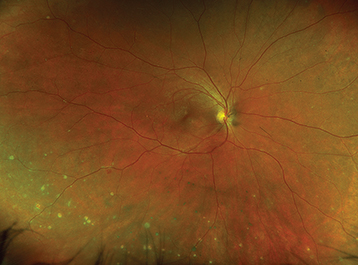
Sarcoidosis: Most frequent systemic disease associated with panuveitis. Key signs include granulomatous KP, iris nodules, trabecular meshwork nodules, peripheral anterior synechiae, vitritis, focal or multifocal initially creamy-appearing choroidal granulomas that progress to atrophic punched-out appearing lesions. May also be associated with optic nerve granulomas, retinal vasculitis (classically a phlebitis with “candle-wax drippings”) which may be occlusive and complicated by peripheral retinal neovascularization (see Figure 12.4.1).
VKH syndrome: Panuveitis characterized by a diffuse choroiditis and multifocal serous retinal detachments. Often has a prodromal phase which resembles a viral illness and includes headaches, fever, and photophobia followed by a uveitis stage. See 12.7, Vogt–Koyanagi–Harada Syndrome.
Sympathetic ophthalmia: Bilateral granulomatous panuveitis with a history of penetrating trauma or intraocular surgery (most commonly vitreoretinal surgery) in one eye; antecedent injury usually occurs 4 to 8 weeks before, but ranges from days to decades, with 90% occurring within 1 year. Posterior segment findings include multiple white-yellow lesions in the peripheral retina (Dalen–Fuchs nodules) and diffuse thickening of the choroid. No current definitive literature to support enucleation of traumatized eye as a preventative measure (unless eye is unsalvageable). Enucleation after development of sympathetic ophthalmia appears to have no benefit. Treatment includes high-dose oral steroids followed by long-term local steroids or systemic immunosuppression. Prognosis in patients with adequate treatment can be good, with 81% of eyes seeing ≥20/40 in one study.
Lens related: Immune reaction to lens material, often secondary to aborted or incomplete cataract extraction, trauma with lens capsule violation, or hypermature cataract. See 9.11, Lens-Related Glaucoma.
Behçet disease: In its most severe form, it can cause a panuveitis. Classic triad of painful oral ulcers, genital ulcers, and uveitis. A skin rash is also common (pathergy—formation of a pustule on skin after needle puncture). Hypopyon uveitis is found in 5% to 15% of patients with uveitis. Aggressive treatment is required as the vasculitis associated with Behçet disease can cause profound ischemia and vision loss. See 12.5, Retinal Vasculitis.
Tattoo-associated uveitis: Pleomorphic uveitis which may be related to systemic sarcoidosis. Associated with induration and itching of tattooed but not adjacent skin. Posterior synechiae and resistance to steroid therapy are common. Often requires immunosuppressive therapy. Removal of preexisting tattoos is not usually effective and often not feasible.
Obtain a thorough history and review of systems. In particular, ask about a history of sexually transmitted diseases, high-risk sexual activity, intravenous drug use, new tattoos or changes in tattoo appearance, prior eye surgery, prior eye surgery or trauma, ringing in ears, headaches, difficulty breathing, rash, and ulcers (oral or genital).
Complete ocular examination, including an IOP check, gonioscopy, and a dilated fundus examination.
Consider OCT to determine lesion location (intraretinal, subretinal, choroidal) and associated CME.
Consider an IVFA to detect subtle vasculitis, peripheral nonperfusion, peripheral neovascularization, or to monitor response to therapy.
Focused serologic testing based on history and examination.
Treponemal test (syphilis EIA, FTA-ABS, TP-PA), followed by confirmatory nontreponemal test (RPR, VDRL). See 12.10, Syphilis.
Interferon gamma releasing assay (IGRA, QuantiFERON Gold) and/or PPD. Consider chest imaging (CXR or CT chest) to assess for signs of active or prior pulmonary disease.
Serologic testing for antibodies against HSV, VZV, and toxoplasmosis can be useful in ruling out a disease as the causative etiology (IgG and/or IgM negative). The presence of positive IgG titer is not necessarily indicative of active disease, but rather prior exposure. Very elevated IgG titers may make you more suspicious for active disease, and a positive IgM indicates recent infection, but again are not fully diagnostic. Negative testing can help rule out disease.
Consider blood cultures to detect bacteremia or fungemia; urinalysis and urine cultures to detect a UTI.
HLA-B51 testing is neither sensitive, nor specific and has minimal clinical utility. Behçet disease is a clinical diagnosis.
Consider an AC paracentesis to detect DNA for CMV, HSV, VZV, or toxoplasmosis-associated disease. See Appendix 13, Anterior Chamber Paracentesis.
Consider a punch biopsy of involved tattooed skin to make a pathologic diagnosis of tattoo-associated uveitis.
Consider topical prednisolone acetate 1% or difluprednate 0.05% q1–2h while awaiting workup results.
Treat infectious etiologies with appropriate antimicrobials prior to using local long-acting steroids or systemic steroids.
Oral acyclovir 400 mg five times per day or valacyclovir 500 mg t.i.d for HSV-associated disease. Oral acyclovir 800 mg five times per day or valacyclovir 1000 mg t.i.d for VZV-associated disease.
For syphilis treatment, see 12.10, Syphilis.
For toxoplasmosis treatment, see 12.9, Toxoplasmosis.
For TB treatment, refer the patient to an internist, infectious disease specialist, or public health officer for consideration of systemic treatment. Patients with ocular TB frequently have no pulmonary disease but still require systemic four-drug antituberculous therapy. Concomitant oral steroids or steroid-sparing immunosuppression may be necessary.
Consider a trial of oral steroids after appropriate negative infectious workup.
Consider local steroid injection, particularly if the disease is unilateral, the eye is pseudophakic, and there is no history of steroid response ocular hypertension.
If the disease becomes persistent consider long-acting local steroids (0.19 mg or 0.59 mg fluocinolone acetonide implants) versus systemic steroid-sparing immunosuppression (e.g., antimetabolites, calcineurin inhibitors, and anti-TNF agents).